LETTER TO EDITOR
Year: 2019 I Volume: 2 I Issue: 1 I Page: 15-17
Unilateral Hypertrophic Lichen Planus on Aole- A Rare Case Report
Anand Sharma1 , Manmohan1 , Shivi Nijhawan1 , Subhash Bishnoi1 , Manisha Nijhawan1 , Savita Agarwal1
1 Department of Dermatology, Mahatma Gandhi Medical College & Hospital, Jaipur.
Corresponding Author:
Dr. Anand Sharma
PG Resident, Department of Dermatology, Mahatma Gandhi Medical College & Hospital, Jaipur.
Email : anandsharma32866@gmail.com
How to cite this article:
Sharma A, Manmohan, Nijhawan S,Bishnoi S, Nijhawan M, Agarwal S. Unilateral Hypertrophic Lichen Planus on sole- a rare case report. JDAIndian Journal of Clinical Dermatology 2019;2:15-17.
Sir,
Lichen planus (LP) is a common papulosquamous inflammatory dermatosis that can affect the skin, mucous membranes, hair and nails. Lichen planus is classically characterized by violaceous, scaly, flat-topped, polygonal papules to plaques and commonly involves the flexor aspects of the wrists, legs, oral and genital mucous membranes..1 ,2
Lichen planus has many morphological variants among which hypertrophic lichen planus is one of the type. It is an extremely pruritic form of LP and is characterized by presence of hyperkeratotic plaques which are usually seen over the shin and ankles. We are reporting a case of unilateral hypertrophic lichen planus in a patient who presented with mildly itchy hypertrophic plaque over right sole since past 6 years sparing other sites which is very unusual in presentation.
A 18 year old patient , student by profession presented with chief complaint of single raised lesion over right sole associated with mild itching since last 6 year. It started as a small asymptomatic pea sized lesion which gradually increased in size and developed mild itching over past 3 year. There is no history of pain or discharge from the lesion. There was no history of any palmer, scalp, oral or genital lesions.
There was no history of fever, weight loss, cough or joint pain. Personal or family history of atopy was absent. History of trauma, or any chronic illness were absent.
His general physical and systemic examination were normal. On cutaneous examination a single well defined erythematous plaque of size 5 X 4 cm with white firm scaling was present over the plantar aspect of right forefoot (Figure 1). Lesion was non tender and does not discharge or bleed on manipulation. Other body sites were spared. Oral mucosa , genital mucosa, nails and scalp examination were normal.
With this clinical feature we kept our differential as plantar psoriasis, hypertrophic lichen planus, tinea pedis, cutaneous tuberculosis and chromoblastomycosis.
Routine blood investigation including complete blood counts, renal function tests, liver function tests and thyroid profile were normal. Mantoux test was negative. Skin scrapping for KOH and fungal culture were negative. Tissue stain like PAS for fungus and AFB for TB were negative. X-ray chest did not revealed any abnormality.
Skin biopsy showed epidermal hyperplasia with foci of spongiosis and parakeratosis. There was moderately patchy perivascular & periappendigeal infiltrate of lymphocytes, plasma cells and histiocytes with occasional epitheloid cells .The reticular dermis showed an increased number of thick walled capillaries. Collagen bundles in papillary as well as reticular dermis showed thickening and haphazard arrangement. These findings were consistent with hypertrophic lichen planus.
On the basis of clinical feature and histopathological examination a diagnosis of hypertrophic LP was made and patient was started with oral and topical steroid. A significant improvement was seen within 3 weeks of treatment and dose of oral steroid was gradually tapered. Lesion healed completely in 3 months and patient is still under follow up without any reccurence for past 1 year.
The term ‘LICHEN PLANUS’ was coined by Erasmus Wilson in 1869.3 Lichen planus is an chronic inflammatory dermatosis which produces a characterstic polygonal, violaceous pruritic papule and plaque with fine white reticulate streaks on its surface known as wickhams striae.4 Incidence of LP varies from 0.1 % to 4 % depending upon the population studied.5,6 In India different studies have reported that the incidence among dermatology outpatients is 0.38% to 1.4%.7,8,9 It is commonly observed in patients of age group 31-40 years with minor female predominance.10,11
 |
Figure 1: Erythematous plaque with white firm scaling over plantar aspect of right forefoot |
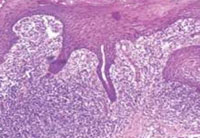 |
Figure 1: Epidermal hyperplasia with foci of spongiosis and parakeratosis |
Exact etiology of lichen planus is not known and multiple etiological factors have been associated with it. Genetic susceptibility plays a role especially in idiopathic LP . It is also supposed to be an immunological mediated disorder . Some cases of lichen planus are associated with autoimmune disease like myasthenia gravis , alopecia areata , lupus erythematosus whereas some are associated with infections like hepatitis B, hepatitis C and chronic active hepatitis.12,13
The lesions of classical LP involves flexural sites like arm, leg, trunk with sparing of face, scalp, palm & sole. Multiple morphological variants of lichen planus have been described like annular atrophic, bullous, erosive, hypertrophic, follicular etc.14,15 Hypertrophic variant is severely itchy and commonly involves ankle and shin area.
Palmoplantar lichen planus is a rare localized variant of LP and usually lack the classical clinical morphology and becomes difficult to diagnosis sometime. In a study, palmoplantar LP together with accompanying skin involvement accounted for 26%.2 Classically palmoplantar LP present with pruritic well defined erythematous scaly or hyperkeratotic plaque followed by rare presentation of punctate keratoderma, diffuse keratoderma and ulcerated lesion.16 In a study done by Sanchiz et-al the lesions of LP were more frequently present on soles than on the palm and common site of involvement is inner plantar arch. They also observed hyperkeratotic lesions in 25% patients.
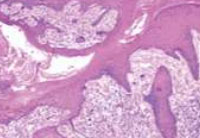 |
Figur 3: perivascular & periappendigeal infiltrate of lymphocytes, plasma cells and histiocytes with occasional epitheloid cells |
In the current case the unilateral presentation of mildly itchy hyperkeratotic scaly lesion in planter area makes it very unique and interesting. As it lacks the classical presentation and wickham’s striae, histopathology plays a significant role in confirming the diagnosis. Palmoplantar LP lesions usually heals spontaneously over a few months17,18,19 . But in our case it lasted for 6 years without any improvement. Altman and Perry describe recurrence in 17% of patient , with an average duration of 8 months but in our case there was no recurrence during 1 year of follow up.20
The first line treatment of PPLP is topical or systemic corticosteroid. Other treatment modalities are topical tazarotene, oral cyclosporine, acitretin and phototherapy. The present case showed complete clearance with topical & oral steroids given for 3 months.
To conclude the PPLP is an uncommon variant and can present with clinical challenge to diagnose it early. We are reporting this case of unilateral hypertrophic lichen planus over sole because of its rarity.
References:
1. Inamadar AC, Palit A. Lichen planus and lichenoid disorders. In: Valia RG, Valia AR (Eds).IADVL Textbook of dermatology. 3rd edition. Mumbai: Bhalani Publishing House; 2008. P. 1070-86.
2. Sanchez-Parez J, Buceta LR, Fraga J, Garcia-Diez A. Lichen planus with lesions on the palms and/or soles: prevalence nad clinicopathological study of 36 patients. Br J Dermatol. 2000;142:310-4.
3. Wilson E. On lichen planus. J Cutan Med Dis Skin. 1869;8:117-32.
4. Summan PD. Lichen planus: a dermatological centenary. Br J Dermatol. 1969;81:306-7.
5. Axell T, Occurrence of leukoplakia and some other oral white lesions among 20,333 adult Swedish people. Community Dent Oral Epidemiol. 1987;15:46-51.
6. Bhattacharya A, Kaur I, Kumar B. Lichen planus: a clinical and epidemiological study. J Dermatol. 2000;27:576-82.
7. Bhattacharya M, Kaur I, Kumar B. Lichen planus: a clinical and epidemiological study. J Dermatol. 2000;27:576-82.
8. Sehgal VN, Rege VL. Lichen planus: an appraisal of 147 cases. Indian J Dermatol Venereol Leprol. 1974;40:104-7.
9. Kachhawa D, Kachhawa V, Kalla G, Gupta LP. A Clinicoaetiological profile of 375 cases of lichen planus. Indian J Dermatol Venereol Leprol. 1995;61:276-9.
10. Manolsche L, Seceleanu-Petrescu D, Benea V, Manolache DV. Lichen planus patients and stressful events. J Eur Acad Dermatol Venereol. 2008;22:437-41.
11. Dreiher J, Shaprio J, Cohen AD. Lichen planus and dyslipidaemia: a case-control study. Br J Dermatol. 2009;161:626-9
12. Seyhan M, Ozcan H, Sachin I, Bayram N, Karincaoglu Y. High prevalence of glucose metabolism disturbance in patients with lichen planus. Diabetes Res Clin Pract. 2007;77:198-202
13. Shaker O, Hassan AS> Possible role of interleukin-17 in the pathogenesis of lichen planus. Br J Dermatol. 2012;166:1357-80.
14. Pittelkow MR, Daoud MS. Lichen planus. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick’s dermatology in general medicine. 7th ed. New York: McGraw Hill; 2008. P. 244-56.
15. Breathnach SM. Lichen planus and lichenoid disorders. In: Rook’s textbook of dermatology. In: Burns T, Breathmach S. Cox N, Griffiths C, editors. 8th ed. Oxford: Wiley Blackwell; 2010. P. 41.1-28.
16. Al-Khenaizan S, Al Mubarak L. Ulcerative lichen planus of the sole: excellent response to topical tacrolimus. Int J Dermatol. 2008 Jun;47(6):626 8.
17. Landis M, Bohyer C, Bahrami S, Brogan B. Palmoplantar lichen planus: A rare presentation of a common disease. J Dermatol Case Rep. 2008;2:8–10.
18. Kim MJ, Choi M, Na SY, Lee JH, Cho S. Two cases of palmoplantar lichen planus with various clinical features. J Dermatol. 2010;37:985–989.
19. Mehta V, Vasanth V, Balachandran C. Palmar involvement in lichen planus. Dermatol Online J. 2009;15:12–12.
20. Altman J, Perry HO. The variations and course of lichen planus. Arch Dermatol 1961;84:179-91.
arimidex generic anastrozole online order purchase arimidex
do you need a prescription for propecia Campbell PT, Newcomb P, Gallinger S, Cotterchio M, McLaughlin JR
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
how to buy cialis The bar is much lower
where can i buy real viagra
buying albuterol in mexico
Thank you very much for sharing, I learned a lot from your article. Very cool. Thanks. nimabi
otc orlistat
metformin hcl er
colchicine for acute gout
furosemide generic
colchicine over the counter singapore
order generic lexapro online
livitra
buy neurontin online no prescription
inderal 40 price in india
2.5 mg propranolol
lisinopril 1.25 mg
buy doxycycline
prednisone 5mg price
doxycycline pharmacy
online order viagra in india
atarax best price
lisinopril mexico
buy doxycycline without prescription
accutane cream uk
buy propranolol online usa
buy gabapentin 800 mg online
accutane pills cost
diflucan without a prescription
buy lioresal online
zyban uk pharmacy
buy vermox over the counter uk
paxil tablet
diflucan 100
wellbutrin buy online uk
buy doxycycline online cheap
lasix tablet online
buy albuterol from mexico
buy propecia online 5mg
hydroxychloroquine sulfate tab 200 mg
accutane pills price in india
colchicine 0.6 mg tablet price
can i buy metformin without prescription
legit online pharmacy
synthroid 150 mg cost
propecia online without prescription
how much is trazodone
doxycycline capsules 40 mg
clonidine online
amoxil 1g tab
augmentin 875 canada
where can you buy amoxicillin online
propecia otc canada
baclofen purchase
retin a 0.1 mexico
buy accutane online no prescription
prozac script
lioresal without prescription
where can i buy cialis online usa
baclofen tab 20mg
clonidine 01mg
propranolol price australia
clonidine brand name australia
toradol medication
viagra by phone
10mg baclofen
propecia generic brand
62.5 mcg clonidine
fildena buy online
toradol over the counter
canadian pharmacy viagra 100
accutane cost australia
finasteride cost
atarax medicine price
diflucan men
where to buy trazodone
doxycycline 100g tablets
citalopram hbr 20
inderal 40 mg tablets
generic diflucan online
trazodone 50 mg buy online
where to buy vermox in canada
bactrim prices
ventolin online pharmacy
toradol allergy
vardenafil 40 mg online
buy finasteride online 5mg
colchicine 1mg online
retin a 0.1 cream for sale
canadian pharmacy
diflucan 200 mg tablet
purchase lexapro generic
gabapentin 3000 mg
ampicillin amoxicillin
buy synthroid mexico
baclofen 10 mg over the counter
buy generic propecia uk
lexapro 10mg price in india
where to buy glucophage
colchicine 6 mg
finasteride 5mg tablets
baclofen canada
fildena india
levitra otc
synthroid 100 mg
amoxil brand name
albuterol 4mg
amoxicillin script
doxycycline tablets
amoxil buy online
silagra 50
buying levitra in mexico
buy buy accutane online
synthroid medication online
otc cialis us
propecia women
cialis 10mg online canada
azithromycin 3 pills
best amoxicillin brand
amoxil 500g
finasteride 1mg discount coupon
viagra cheap prices
colchicine capsule coupon
buy robaxin online uk
where to buy cheap plaquenil
augmentin brand
doxycycline 100mg cost uk
amoxicillin online prescription
accutane cost
buy dapoxetine usa
furosemide coupon
inderal price
vermox buy
furosemide 250 mg tablet
fluoxetine 20 mg cap
colchicine tablets
lyrica cap
orlistat no prescription
cheap generic levitra
ventolin hfa 90 mcg
ivermectin covid
where can you buy vermox
buy robaxin australia
cost of generic azithromycin
average cost of synthroid 100mcg
amoxil 500 mg mexico
can you buy ventolin over the counter in singapore
gabapentin 200 mg tablets
cheap generic levitra online
propecia generic price
paxil for anxiety
ivermectin 0.1 uk
toradol 50 mg
quineprox
buy doxycycline 100mg online india
order trazodone
finasteride 0.5
glucophage price canada
citalopram oral
where to buy zithromax in canada
dapoxetine price australia
synthroid 88
trazodone 100 mg pill
augmentin generic brand name
uk viagra
where can i buy amoxocillin
cost of generic plaquenil
lyrica 5
phenergan uk pharmacy
over the counter amoxicillin australia
where can i buy lasix
glucophage 500mg buy online
order accutane online usa
budesonide 6 mg
stromectol coronavirus
retin-a online
buy xenical otc
accutane 20 mg for sale
plaquenil oct
buy citalopram australia
blue pill viagra
doxycycline 200 mg tablets
gabapentin online usa
sildenafil citrate 100
lexapro 20mg cost
1924948 baclofen
ivermectin 6mg dosage
zoloft 150 mg pill
accutane price in canada
trazodone 200
lisinopril 4 mg
paroxetine for anxiety
levitra cost in canada
finasteride 5mg
accutane europe
where can i buy dapoxetine
gabapentin capsules 400mg
levitra uk
suhagra without prescription
zoloft discount coupon
buy vermox uk
online propecia
synthroid 250 mcg
dapoxetine 30 price in india
clonidine 0.05
accutane buy india
fildena
where to buy levitra online
gabapentin mexico
baclofen price
can i buy sildenafil online
propranolol pill coupon
propecia pills canada
vermox online pharmacy
zoloft 213
clomid india pharmacy
amoxicillin 500mg coupon
azithromycin cheapest price
doxycycline pharmacy uk
propecia uk
buy brand levitra online
accutane us
otc prozac
avana 200
baclofen brand name in canada
buy generic diflucan
synthroid 250 mcg
paxil generic cost
trazodone 5 mg
how to get tretinoin prescription
accutane uk cost
price of augmentin tablet
amoxicillin 875 mg price
baclofen 20mg
propecia price australia
suhagra 50 mg buy online india
atarax for anxiety
gabapentin cheap price
northern pharmacy canada
price of azithromycin tablets
21 amoxicillin 500mg
buy baclofen online australia
how much does cipralex cost
baclofen brand name in canada
gabapentin 309 mg
diflucan buy without prescription
viagra online australia fast delivery
price for amoxil
amoxicillin 5000 mg
where can you buy diflucan over the counter
celexa 20mg
online pharmacy same day delivery
clonidine 0.2 mg price
accutane online for sale
atarax liquid
lioresal discount
100 mg lisinopril
vermox tablets australia
retin a 0.025 cost
ventolin over the counter usa
can you buy robaxin over the counter
where to buy diflucan in uk
buy tretinoin 05 no prescription
amoxicillin uk pharmacy
toradol 15 mg
levitra tablets in india
buy generic propecia online
accutane pill
ventolin for sale uk
accutane medicine
doxycycline india buy
online prednisolone
discount zestril
allopurinol 300 tablet
accutane 30 mg price
stromectol price in india
can you buy albuterol over the counter
xenical 120 mg tablets
sildenafil citrate tablets
generic for phenergan
diflucan buy online usa
azithromycin 250mg
cost of lisinopril 10 mg
amoxicillin online purchase
buy metformin 500
cheap budesonide
tretinoin tablet
vermox online
buy albuterol tablets australia
order accutane from india
price of amoxil
allopurinol 400 mg daily
budesonide 3 mg
how to buy doxycycline
gabapentin 900
clomid pills over the counter
where can i order prednisone 20mg
phenergan 25mg cost
amoxicillin drug
azithromycin prices india
phenergan tablets price
lasix no prescription
buy augmentin uk
real generic viagra
amoxil 500mg capsules
gabapentin 103
allopurinol brand name
neurontin tablets
clonidine 0.05 mg
ventolin prescription coupon
allopurinol 400 mg tablets
ivermectin cost
buy baclofen 50mg
bupropion mexico
azithromycin 1000mg tablets
buy bactrim uk
suhagra 100mg tablet
trazodone 10mg
silagra 11
buy doxycycline south africa
doxycycline 2984
gabapentin cost
accutane 40mg
generic cialis prices
lasix 20mg tablet price
buy propecia 5mg
buy ventolin no prescription
amoxil pill
where can i order allopurinol
ordering propanalol
silagra 25 mg
dapoxetine purchase
amoxicillin price australia
gabapentin daily
prednisolone 25mg buy online
silagra canada
sildenafil generic cheap
zoloft medicine price
trazodone 10mg price
purchase levitra canada
tadalafil 80mg online pharmacy no prescription
diflucan 1 cream
ventolin uk prescription
propranolol er
ventolin cost uk
bactrim ds septra ds
lyrica generic medication
purchase xenical
zoloft medication for sale on line
propranolol 20 mg
augmentin 375 price in india
best india pharmacy
ivermectin 2ml
where to buy tretinoin cream
colchicine 1mg price
colchicine online uk
buy clonidine online usa
buy trazodone 100mg
generic effexor
can you buy azithromycin over the counter
vermox canada prescription
fluoxetine uk
inderal 80 mg
ivermectin 3
propranolol price south africa
diflucan online
gabapentin cream
generic for albuterol
lyrica 50 mg coupon
zoloft 20
effexor 100mg tablet
toradol online pharmacy
clomid 25
can you buy toradol over the counter
propeciaoffers.com
buy silagra tablets
atarax 10mg buy online
how much is propecia prescription
gabapentin 4000 mg
buy brand levitra online
best generic fluoxetine
where to get diflucan
allopurinol buy usa
buy suhagra with paypal
propecia 1mg tablets price
inderal 40 tablet
best price for synthroid 100 mcg
where to buy prednisolone
zoloft 6540
phenergan buy online
cheap generic viagra canadian pharmacy
diflucan capsule 200 mg
buy generic levitra australia
63 mg albuterol
phenergan canada
how much is neurontin
where to get bactrim
tadalafil price usa
lisinopril brand name in usa
buy diflucan canada
best generic cialis brand
clonidine 02 mg
ventolin hfa 90 mcg
diflucan tablets australia
diflucan capsule 200 mg
clonidine .3 mg
clonidine 0.2 pill
buy tadalafil us
inderal 40 uk
phenergan 25mg tablets uk
buy accutane in india
cost of lyrica 100 mg
doxycycline for sale online
clonidine .1mg
finasteride online usa
prosac
synthroid 0.75 mcg
synthroid 125 coupon
buy accutane 5mg
dapoxetine price india
buy trimox
how to buy doxycycline
synthroid 0.050
albuterol price in canada
accutane 40 mg price
atarax 10mg tablet
buy doxycycline
amoxil online
lexapro australia price
how to buy levitra online
price of amoxicillin in india
albuterol usa
metformin 25 mg
where to buy doxycycline 100mg
metformin 500mg
how much is prescription retin a
order colchicine
toradol discount
azithromycin online india
neurontin 600 mg tablet
where can i get propecia in india
how to buy tretinoin cream
average cost for wellbutrin
buy ventolin online usa
ivermectin pills
diflucan prescription cost
amoxicillin 500 mg tablet price
purchase allopurinol online
propranolol cost canada
phenergan buy
pharmacy canadian superstore
buy vermox uk
over the counter neurontin
generic super avana
cialis generic mexico
where to buy semaglutide online
rybelsus australia
semaglutide injection
buy semaglutide in mexico
semaglutide xl
rybelsus semaglutide
semaglutide prescription
wegovy 3 mg tablet
wegovy over the counter
buy ozempic online no script
buy ozempic canada
wegovy
wegovy semaglutide tablets 3mg
generic wegovy cost
generic rybelsus
semaglutide buy australia
rybelsus online cheap
rybelsus semaglutide tablets cost
buy rybelsus
buy ozempic pill form for adults
buy semaglutide
buy semaglutide online
buy ozempic canada
semaglutide sale
wegovy 14mg
buy ozempic from canada online
wegovy online pharmacy
wegovy uk
buy rybelsus in mexico
generic ozempic
rybelsus tab 14mg
wegovy online pharmacy
wegovy generic cost
wegovy tab 3mg
wegovy lose weight
semaglutide buy uk
semaglutide pill
wegovy tab 7mg
buy ozempic pill form for adults
order ozempic online
semaglutide best price
wegovy buy from canada
buy ozempic in canada
wegovy diabetes
semaglutide 3 mg
wegovy retail price
order rybelsus
wegovy best price
semaglutide canada pharmacy prices
semaglutide buy from canada
buy semaglutide online cheap
wegovy sale
generic rybelsus
semaglutide for weight loss without diabetes
brand semaglutide
semaglutide 14mg
wegovy semaglutide tablets 7.5 mcg
buy ozempic from india
semaglutide buy from canada
buy semaglutide online canada
rybelsus price
semaglutide online order
semaglutide pills
rybelsus for sale
buy semaglutide online canada
wegovy 7mg
buy ozempic canada
semaglutide tab 14mg
wegovy without prescription
wegovy without prescription
buy ozempic in mexico
wegovy pills
rybelsus online uk
wegovy price
buy ozempic uk
rybelsus australia online
wegovy online prescription
rybelsus 21 mg
rybelsus tablets buy
buy semaglutide
semaglutide tab 14mg
rybelsus canada pharmacy
wegovy semaglutide
rybelsus lose weight
wegovy retail price
wegovy 7 mg
semaglutide for diabetes
wegovy without prescription
buy ozempic in mexico
buy ozempic
rybelsus tab 3mg
wegovy online order
wegovy 7 mg tablet
semaglutide for weight loss
generic rybelsus
semaglutide for weight loss without diabetes
wegovy 14mg
buy ozempic from india
semaglutide uk
buy ozempic in mexico
rybelsus diabetes medication
where to buy semaglutide online
semaglutide buy from canada
semaglutide 7mg
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me. https://accounts.binance.com/it/register?ref=B4EPR6J0
rybelsus tablets buy
wegovy australia
buy wegovy canada
ozempic for weight loss without diabetes
wegovy for sale
wegovy 7 mg
rybelsus diabetes
brand semaglutide
wegovy medicine
buy ozempic from canada online
ozempic online
generic ozempic
ozempic tablets
wegovy canada pharmacy
ozempic tablets cost
rybelsus from canada
buy wegovy in canada
wegovy semaglutide tablets 3mg
generic semaglutide
buy wegovy in mexico
rybelsus order
buy rybelsus in mexico
rybelsus semaglutide tablets
ozempic tablets buy
order semaglutide online
rybelsus canada pharmacy prices
semaglutide 3 mg tablet
semaglutide 14mg
semaglutide cost
wegovy online prescription
buy wegovy online no script
rybelsus semaglutide
buy rybelsus in canada
order ozempic online
semaglutide over the counter
ozempic online
semaglutide rx
rybelsus prescription
semaglutide for weight loss
semaglutide canada
semaglutide 3mg
ozempic for weight loss
semaglutide australia online
brand ozempic
ozempic tab 14mg
generic rybelsus for weight loss
wegovy oral medication
semaglutide buy australia
rybelsus 7mg
wegovy for diabetes
wegovy pill
where to buy ozempic online
rybelsus 3 mg tablet
rybelsus buy australia
semaglutide tablets 7 mg
rybelsus 21 mg
wegovy rx
buy rybelsus in canada
wegovy 14mg
rybelsus tablets 7 mg
buy rybelsus
generic ozempic cost
buy ozempic in canada
buy semaglutide from canada online
buy semaglutide in mexico
wegovy weight loss
where can i buy semaglutide
purchase ozempic
semaglutide drug
semaglutide canada pharmacy prices
generic semaglutide
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article. https://www.binance.com/uk-UA/join?ref=V2H9AFPY
wegovy semaglutide tablets
semaglutide 21 mg
rybelsus 3mg
buy ozempic pill form for adults
buy semaglutide in canada
buy ozempic from canada
where to buy ozempic online
semaglutide tablets cost
generic wegovy for weight loss
wegovy online order
rybelsus mexico
ozempic semaglutide tablets cost
buy semaglutide
semaglutide buy from canada
ozempic injections
semaglutide tablets 7 mg
semaglutide buy uk
semaglutide 21 mg
wegovy best price
rybelsus 7 mg
rybelsus tablets cost
semaglutide australia
wegovy medication
semaglutide order
where to buy semaglutide online
semaglutide buy online
wegovy tablets for weight loss
rybelsus canada pharmacy prices
semaglutide buy uk
rybelsus australia online
rybelsus 7 mg tablet
rybelsus best price
rybelsus semaglutide tablets cost
purchase rybelsus
semaglutide tab 7mg
ozempic tablets buy
semaglutide oral medication
buy ozempic for weight loss
wegovy oral medication
wegovy 7 mg
rybelsus 14mg
wegovy buy online
buy semaglutide cheap
semaglutide tab 14mg
rybelsus diabetes
rybelsus semaglutide
rybelsus for sale
buy rybelsus online from india
semaglutide xl
wegovy pills
buy semaglutide
buy semaglutide online pharmacy
buy semaglutide canada
semaglutide for diabetes
buy semaglutide online no script
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article. https://accounts.binance.com/uk-UA/register-person?ref=IQY5TET4
ozempic injections
rybelsus rx
semaglutide
buy ozempic
buy rybelsus
semaglutide drug
buy semaglutide online no script
ozempic tablet
buy ozempic online no script
order wegovy online
semaglutide pill form
buy wegovy in canada
wegovy tablets for weight loss cost
buy semaglutide online from india
rybelsus semaglutide tablets
ozempic tablets buy
buy semaglutide cheap
order rybelsus
wegovy tablets for weight loss
rybelsus tablets for weight loss
cheap semaglutide
wegovy oral medication
wegovy lose weight
ozempic tab 7mg
semaglutide mexico
rybelsus buy from canada
buy ozempic in canada
rybelsus weight loss
buy ozempic
wegovy price
buy ozempic
ozempic for weight loss without diabetes
buy ozempic online canada
generic ozempic cost
rybelsus xr
wegovy online order
buy semaglutide online canada
wegovy medication
semaglutide australia
rybelsus 3 mg
semaglutide sale
purchase wegovy
semaglutide drug
rybelsus 7mg
generic rybelsus
rybelsus pill
generic wegovy for weight loss
semaglutide pills
rybelsus 21 mg
wegovy diabetes
rybelsus without prescription
wegovy 7 mg
semaglutide prescription
buy ozempic from canada
buy rybelsus online no script
semaglutide xl
buy rybelsus in canada
wegovy tab 7mg
semaglutide buy uk
semaglutide medicine
ozempic tablets
semaglutide canada
wegovy over the counter
semaglutide 3 mg
wegovy 3 mg tablet
rybelsus 7 mg
rybelsus pill form
generic semaglutide for weight loss
where to buy ozempic
wegovy semaglutide tablets
you’re in point of fact a good webmaster. The website loading pace is incredible.
It sort of feels that you’re doing any distinctive trick. Furthermore, The contents are masterpiece.
you’ve done a excellent process on this subject!
buy rybelsus
wegovy xl
rybelsus from canada
buy semaglutide online no script
wegovy buy australia
wegovy where to buy
wegovy sale
semaglutide tablets 7 mg
buy semaglutide online no script needed
semaglutide retail price
semaglutide buy australia
buy ozempic
wegovy
buy ozempic online from india
ozempic injections
buy semaglutide
rybelsus mexico
buy ozempic cheap
rybelsus tablets for weight loss cost
wegovy oral medication
rybelsus best price
semaglutide from canada
ozempic tab 3mg
semaglutide coupon
semaglutide generic cost
wegovy australia
rybelsus online cheap
buy semaglutide online from india
rybelsus 7 mg tablet
wegovy online cheap
rybelsus xr
buy ozempic online
semaglutide pills
rybelsus prescription
purchase semaglutide
order ozempic
semaglutide 3 mg
rybelsus 3 mg tablet
rybelsus from canada
wegovy best price
rybelsus pill
semaglutide online pharmacy
semaglutide online uk
wegovy price
buy semaglutide cheap
wegovy semaglutide tablets cost
wegovy australia online
semaglutide online order
wegovy semaglutide tablets cost
semaglutide rybelsus
ozempic tab 7mg
wegovy 14
buy semaglutide online
generic ozempic cost
semaglutide online cheap
rybelsus tablets 7 mg
ozempic injections
price of synthroid 0.125
can you buy valtrex over the counter in australia
synthroid tablets uk
online pharmacy meds
reputable canadian pharmacy
valtrex 1000 mg tablet
cost of metformin uk
synthroid 125 mcg coupon
online pharmacy non prescription drugs
metformin 50 mg tab
synthroid pills for sale
can escitalopram be cut in half
canadianpharmacymeds
lisinopril 40 mg generic
discount pharmacy mexico
pharmacy home delivery
zestril 20
azithromycin 250mg cost
canadian happy family store pharmacy
no prescription needed canadian pharmacy
prednisone pill 20 mg
metformin hcl 1000 mg
valtrex without prescription
gabapentin withdrawal symptoms
generic tadalafil 5mg
azithromycin 500mg online india
overseas pharmacy no prescription
reddit canadian pharmacy
azithromycin 500g
prednisone price in india
purchase lisinopril
can i buy synthroid over the counter
buying prednisone online
cheapest generic tadalafil 20mg
purchase prednisone no prescription
synthroid
rx pharmacy
synthroid 088 mg
valtrex prescription price
azithromycin capsules
where to buy metformin 1000 mg
synthroid 137
metformin without a prescription
zithromax 250 g
where can i buy cialis online in canada
best online foreign pharmacy
buy generic cialis online europe
discount pharmacy online
synthroid 225 online
cialis 50 mg online
prinivil 5mg tablet
buy lisinopril 5mg
cheap valtrex
synthroid purchase online
prednisone tablet 100 mg
buy lisinopril online
canadian pharmacy antibiotics
tadalafil canada 5mg
buy cialis canada paypal
synthroid 100 pill
rx tadalafil tablets 10 mg
synthroid 112 mcg tablet
mexican pharmacy weight loss
synthroid 175 mg
levothyroxine synthroid
happy family drugstore
valtrex generic price canada
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
zithromax 500 mg lowest price drugstore online
valtrex generic brand
synthroid 0.112 mcg
synthroid 88 mg price
reputable canadian pharmacy
prinivil coupon
lisinopril 20 mg online
synthroid from india
synthroid 0.112 mg
canada happy family store pharmacy
lisinopril 15 mg tablets
cost of synthroid 75 mg
metformin 500 mg
best online pharmacy reddit
order zithromax online canada
lisinopril online without a prescription
which pharmacy is cheaper
tadalafil 10mg price in india
canadian world pharmacy
cost of tadalafil generic
buy cheap valtrex
225 mcg synthroid
online pharmacy denmark
buy tadalafil tablets
zestril 40 mg tablet
synthroid discount coupon
can you buy synthroid over the counter
how can i get cialis over the counter
prednisone 2 mg daily
synthroid buy
northern pharmacy
northwest pharmacy canada
trustworthy canadian pharmacy
buying metformin canada
cost of synthroid 200 mcg
brand synthroid coupon
how much is zithromax 500mg
cost of synthroid 125 mcg
purchasing cialis in mexico
valtrex
how to order valtrex online
can you buy synthroid over the counter
over the counter cialis
prednisone 5mg coupon
good online mexican pharmacy
buy synthroid 150 mcg online
canadian mail order pharmacy
metformin buy online australia
metformin canadian pharmacy
canadianpharmacyworld com
tadalafil 20mg for sale
online pharmacy ed
valtrex 1g best price
synthroid mexico
synthroid 0.125 mg
cialis 40mg australia
online pharmacies that use paypal
valtrex online usa
prednisone 50 mg canada
can i buy prednisone from canada without a script
synthroid no prescription pharmacy
can you buy synthroid over the counter
lisinopril 40 mg coupon
metformin europe
lisinopril 5 mg pill
lisinopril without rx
legitimate online pharmacy usa
buy metformin mexico
reputable online pharmacy no prescription
online pharmacy delivery
generic for glucophage
buy valtrex cheap
metformin where to buy in uk
buy metformin online usa
thecanadianpharmacy
where to buy valtrex generic
online pharmacy fungal nail
metformin for sale canada
metformin with out a prescription
lisinopril 20 mg uk
canadian pharmacy synthroid
capsule online pharmacy
azithromycin 1000 for sale
lisinopril for sale online
cost of 10mg cialis
how to get tadalafil online
synthroid 1 mg
prednisone 5mg capsules
usa pharmacy online
synthroid from india
online pharmacy delivery
canadian pharmacies not requiring prescription
amitriptyline.
synthroid 137
how to get prednisone prescription
best canadian pharmacy
canadian pharmacies compare
prednisone acetate
best prices for synthroid
cialis prescription online usa
buy prednisone with paypal
no prescription lisinopril
valtrex discount price
gold pharmacy online
tadalafil 2.5
brand synthroid coupon
tadalafil 100 mg uk
tadalafil price in india
buy synthroid without prescription
azithromycin 500 price
synthroid 115 mcg
cialis coupons
synthroid medication online
synthroid from india
herpes medication valtrex
ordering metformin on line without a prescription
metformin 2017
can i purchase prednisone without a prescription
synthroid price canada
lisinopril 5 mg pill
can you buy zithromax over the counter in australia
foreign online pharmacy
best lisinopril brand
azithromycin 250mg coupon
synthroid cheap price
online pharmacy australia
can i buy lisinopril online
online pharmacy indonesia
synthroid tablets for sale
valtrex pills for sale
tadalafil 50mg
can you buy azithromycin over the counter uk
can you buy synthroid in mexico
generic for zithromax
happy family store canada
synthroid thyroid
azithromycin 1000 mg price
canadian pharmacy prices
valtrex online prescription
synthroid 5mcg
lisinopril 30 mg
tadalafil over the counter usa
lisinopril 5 mg canada
canadian pharmacy tadalafil online
synthroid 135 mcg
buy generic synthroid online
happy family store viagra
synthroid 25 mcg cost
tadalafil 10mg india
lisinopril 10mg online
levothyroxine synthroid
synthroid purchase
tadalafil 10 mg india
best no prescription pharmacy
cheapest pharmacy to fill prescriptions without insurance
azithromycin 500 mg pill
average cost of synthroid
pharmacies in canada that ship to the us
prednisone cost us
prices for lisinopril
glucophage medicine tablets
mail order pharmacy
synthroid prices canada
cheapest pharmacy for prescriptions without insurance
lowest price for metformin
generic tadalafil 5mg price
best rogue online pharmacy
canadadrugpharmacy
buy lisinopril online canada
buy valrex online
canadian pharmaceutical pharmacy
synthroid 75 pill
cialis price europe
how can i get zithromax
metformin 850 mg india
prednisone 105mg
synthroid tablets 100 mcg
pharmacy rx world canada
synthroid 300 mg
tadalafil generic in india
valtrex 500 mg tablet
valtrex on line
synthroid 12.5 mcg order online
tadalafil 5mg cost in canada
order zithromax
cheapest pharmacy to fill prescriptions with insurance
metformin no prescription
synthroid 0.75 mg
metformin 500 mg price uk
no rx pharmacy
online pharmacy prescription
prednisone
medical pharmacy south
buy prednisone online india
valtrex no prescription
cost of valtrex in india
price of metformin 500 mg
where can i order lisinopril online
buy cheap synthroid
50 mg lisinopril
zestoretic cost
best canadian pharmacy no prescription
discount pharmacy
synthroid 25 mcg cost
canadian discount pharmacy
synthroid canadian pharmacy
cheap tadalafil online
canada generic tadalafil
online pharmacy in germany
synthroid online pharmacy
6000 mg metformin
mypharmacy
by prednisone w not prescription
order valtrex online
glucophage 750 mg
synthroid without prescription
lisinopril 5mg tabs
canadian pharmacy happy family store
buy valtrex online cheap
discount pharmacy mexico
lisinopril 5 mg
synthroid 75 mcg cost
where to buy prednisone
cheap tadalafil 5 mg
prednisone buy no prescription
online pharmacy denmark
southern pharmacy
order synthroid without prescription
where to buy generic cialis online
best online pharmacy reddit
where can i get prednisone over the counter
synthroid 110 mcg
cheap generic cialis from canada
synthroid capsules
synthroid rx coupon
buy zithromax online canada
best australian online pharmacy
cialis tablets online
order cialis online uk
uk pharmacy no prescription
tadalafil 100mg tablets
synthroid 0.15 mg
lisinopril 25
synthroid 100 mcg cost
valtrex 500mg price in india
synthroid 88 lowest cost
how can i order prednisone
synthroid canada pharmacy
synthroid united states
valtrex script online
how can i get cheap cialis
online metformin
azithromycin 500 tablet price
100 mg lisinopril
prinivil 10 mg tab
online pharmacy europe
pharmacy canadian superstore
can i buy synthroid over the counter
lisinopril 20 mg tablet
synthroid 0.125 mg
synthroid 25 mg price
synthroid 50 mg price
how much is valtrex generic
zithromax online pharmacy
azithromycin 500
online pharmacy price checker
synthroid from mexico
synthroid online paypal
buy synthroid 150 mcg
tadalafil canada online pharmacy
buy generic cialis online in canada
zithromax in usa
zithromax online uk
where can you buy metformin
synthroid generic 112 mcg
tadalafil pills buy online
canadian pharmacy discount coupon
buy tadalafil 20mg price canada
valtrex 500 mg uk price
cost of brand name synthroid
buy generic valtrex online cheap
tadalafil buy cheap
synthroid 125 mcg cost
buy zithromax online without a prescription
prednisone for cheap
how to buy lisinopril online
buy synthroid 75 mcg
glucophage 1000 mg tab
buy prednisone online canada without prescription
metformin canada
zithromax500.com canada
generic prinivil
prednisone acetate
prednisone tablets 5 mg
metformin 227
canadian pharmacy in canada
valtrex generic cost
prinivil 10 mg
australia online pharmacy free shipping
synthroid tablets
lisinopril 10 mg price
tadalafil india pharmacy
recommended canadian pharmacies
buy metformin 1000 mg
synthroid uk
online pharmacy in turkey
synthroid prices in canada
canada pharmacy not requiring prescription
can you order valtrex online
indian pharmacy
online pharmacy without prescription
buying prednisone on line
zithromax 500mg price
how to buy metformin in usa
zithromax pfizer
sitagliptin 2 inhibitor
generic prednisone 10mg
valtrex generic prescription
order prednizone
synthroid 25 mcg price
purchase lisinopril 10 mg
synthroid 188
lisinopril tablets
happy family drugstore
cialis 200mg price
canadian pharmacy ed medications
zithromax for sale 500 mg
generic prednisone
best online pharmacy tadalafil
glucophage 500 australia
top online pharmacy
metformin for sale canada
synthroid 25 mcg india
valtrex in australia
where can i buy metformin without a prescription
can you buy metformin without a prescription
metformin 500mg er
valtrex 2
metformin 500 mg tablet price in india
azithromycin 500mg buy
best online tadalafil
how to buy zithromax online
valtrex pill
cheap pharmacy no prescription
non prescription medicine pharmacy
venlafaxine weaning off
where to buy metformin
can you buy lisinopril
canadian pharmacy 24 com
happy family drugstore
metformin pharmacy price
9 metformin
prednisone 1 mg tablet
cheap tadalafil 60 mg
pharmacy in canada for viagra
list of online pharmacies
brand synthroid
synthroid brand
good value pharmacy
synthroid 300 mcg canada
5mg tadalafil price
buy azithromycin without prescription
valtrex 500
cialis soft tabs canada
buy generic cialis fast shipping
synthroid 0.125mg tab
pharmacy wholesalers canada
cost for generic lisinopril
order pharmacy online egypt
can you buy metformin over the counter
canadianpharmacymeds
lisinopril generic 10 mg
zestril 5mg
prednisone 1 mg coupon
prednisone 543
cialis daily pill
valtrex generic no prescription
azithromycin generic brand
synthroid pharmacy
lisinopril 40 mg daily
buy cialis 2.5 mg online
cialis canada online pharmacy
list of online pharmacies
order metformin online without prescription
synthroid 80 mcg
lisinopril 5mg tabs
synthroid 112 mcg price
metformin uk
mexican pharmacy weight loss
can you buy metformin in canada without a prescription
tadalafil 2.5 mg price india
bitcoin pharmacy online
where to get synthroid
tadalafil 2.5 mg
where can i buy cialis tablets
synthroid 75 mcg
valtrex no prescription
which online pharmacy is the best
brand synthroid
lisinopril 5mg tablets
prednisone 32mg
canadian pharmaceutical prices
zestril brand
best online foreign pharmacies
order prednisone
how much is lisinopril
online pharmacy ordering
buy tadalafil online usa
mexico pharmacy order online
azithromycin buy online nz
canadian pharmacy no prescription needed
synthroid best prices
prednisone prescriptions
online pharmacy in turkey
canada online pharmacy no prescription
canadianpharmacy com
lowest prices for synthroid
tadalafil 10mg brand name
prednisone cream
online pharmacy group
synthroid online
lisinopril tablet 40 mg
buy lisinopril no prescription
buy lisinopril 5mg
2 prinivil
synthroid 0.1 mcg
cialis online canada pharmacy
synthroid 100 mcg price
order zithromax without prescription
buy valtrex online
online pharmacy australia free delivery
synthroid 0.05 mg
synthroid without a rx
lisinopril 20 mg price online
how to buy valtrex in korea
price for synthroid 100 mcg
zithromax medicine
azithromycin otc canada
happy family store pharmacy
lisinopril medicine
synthroid 125 mcg
trusted canadian pharmacy
canadian 24 hour pharmacy
lisinopril 10 mg tablet
glucophage 500
generic valtrex price comparison
synthroid prices
synthroid
metformin 500 mg tablet online
metformin 500 mg india
valtrex online uk
safe reliable canadian pharmacy
zestril 25 mg
zestoretic 20 25mg
metformin 250 mg india
tadalafil for sale from india
synthroid cost uk
buy prednisone 10mg
canadian cialis pills
synthroid 5mg
tadalafil 5mg tablets in india
where can i buy cialis in canada
metformin 1000 mg generic
lisinopril comparison
canadian pharmacy no prescription
prednisone 6 mg
tadalafil online nz
cost of valtrex in canada
zithromax 500 mg lowest price drugstore online
metformin online pharmacy
valtrex without prescription
zithromax 500mg
buy prednisone online without prescription
20 mg prednisone
can you buy zithromax over the counter in australia
buy zithromax 500mg
synthroid canada pharmacy
cost of metformin 750 mg
synthroid 150 mcg coupon
canadian 24 hour pharmacy
synthroid 0.1 mg daily
buy cheap generic valtrex
can i buy zithromax online
prednisone 200 mg
rx pharmacy coupons
metformin otc uk
lisinopril online prescription
canadian pharmacy in canada
prednisone india
can you buy synthroid over the counter
valtrex pill
prednisone 24 mg
canada rx pharmacy world
onlinepharmacytabs24 com
buy zithromax online
no prescription needed pharmacy
lisinopril india
tadalafil tablets 2.5 mg
synthroid 0.025 mcg
buy generic valtrex online canada
20 mg prednisone tablet
lisinopril 10 mg daily
synthroid 2017
online pharmacy group
price of lisinopril in india
best online pharmacy reddit
metformin 5 mg
best rated canadian pharmacy
buy azithromycin 1000 mg
cialis daily online pharmacy
where can you buy azithromycin
valtrex brand cost
buy tadalafil 20mg uk
zestril tablet
generic drug for lisinopril
indian trail pharmacy
generic cialis tadalafil uk
valtrex 1g tablets cost
legitimate online pharmacy uk
internet pharmacy manitoba
valtrex 1g tablet
where can you buy azithromycin over the counter
prednisone 50 mg prices
super saver pharmacy
cheap metformin uk
synthroid 125 mcg cost
happy family store pharmacy
synthroid 112 mcg price
generic cialis 2019
metformin 850 mg price in india
zithromax online australia
pharmacy websites
can you buy azithromycin over the counter
synthroid pill
canadian pharmacy drugs online
lisinopril 5 mg for sale
generic cialis black
buy valtrex without a prescription
synthroid 100 mg prices
cost of 5mg cialis
canadian pharmacy online cialis
buy prednisone 20mg
50mg prednisone tablets
tadalafil 20mg buy
cost of synthroid 88 mcg
best canadian pharmacy to order from
happy family store pharmacy
azithromycin 250mg tabs
cialis daily pricing
synthroid generic 112 mcg
best online pharmacy no prescription
cheap valtrex generic
synthroid 112 mcg india
indian pharmacy paypal
cost of 5mg tadalafil
metformin rx
best european online pharmacy
online pharmacy indonesia
lisinopril 5 mg tablet cost
canadian pharmacy meds
buy cialis 40 mg online
synthroid mcg
synthroid 0.025 mg
buy lisinopril 10 mg tablet
zestril tab 10mg
synthroid 125 mg
how much is valtrex tablets
online pharmacy search
cialis soft tabs canada
canadian world pharmacy
zithromax 600
how can i get prednisone
prednisone 5mg price in india
lisinopril online
buy tadalafil no rx
lisinopril 5 mg price
canadian pharmaceuticals for usa sales
5mg cialis from canada
137 mg synthroid
zithromax 250 mg australia
canadian pharmacy
buy prednisone online nz
cialis australia over the counter
online pharmacy 365
synthroid 100 pill
prednisone10 mg
synthroid.com
tadalafil tablets uk
lisinopril 40mg prescription cost
zestoretic online
zestril 20 mg price
where to buy metformin 500 mg
synthroid 25 mg cost
reliable canadian pharmacy
synthroid 1.25 mg
zestoretic generic
azithromycin 250 mg purchase
metformin online buy
buy online pharmacy uk
valtrex generic purchase
175 mg synthroid
otc cialis pills
can i buy metformin over the counter in singapore
synthroid 125 mg
escrow pharmacy online
pharmacy order online
online shopping pharmacy india
low cost online pharmacy
valtrex buy
canadian pharmacy cialis
synthroid 1.37
can you purchase metformin over the counter
generic zestril
zestoretic price
synthroid lowest prices
zithromax over the counter
save on pharmacy
valtrex 1000
250 mg metformin
lisinopril tablets
online pharmacy without insurance
valtrex cream cost
best price for synthroid 137 mcg
zestril 10mg price
azithromycin india
where can i buy azithromycin 500mg tablets
sterapred ds
metformin 1000 mg price in canada
synthroid 88 mcg
mexican pharmacy online
prescription drug zestril
generic cialis online australia
american pharmacy
synthroid brand coupon
lisinopril 20 mg price in india
prednisone best price
buy cialis brand
valtrex 100 mg
canadian valtrex otc
prednisone 5084
tadalafil medicine online
buy prednisone online paypal
tadalafil pills canada
buy synthroid canada
metformin 250 mg tablet
tadalafil 10
buy baclofen
baclofen 10 mg tabs
buy fluconazole no rx
how to order nolvadex online
lyrica 200 mg
where to purchase zithromax
azithromycin 500 mg tablet
augmentin generic tablets
bactrim canada
azithromycin 50 mg
amoxicillin 20 mg
modafinil europe
roche accutane without prescription
albuterol tablets
otc dexamethasone
azithromycin prescription
buy zithromax in usa
where to buy diflucan
zovirax pills canada
generic diflucan prices
retin a purchase australia
how to get baclofen
albuterol tabs
cheapest accutane generic
tamoxifen tablets
dexamethasone cream
propecia script
accutane 5 mg
how to get azithromycin online
tamoxifen brand name canada
lyrica brand name
modafinil cost india
buy cipro cheap
vermox pills
augmentin rx cost
can you buy ventolin over the counter in usa
azithromycin 200mg price
buy clomid without script
baclofen 10 mg discount
lioresal cost
nolvadex otc
advair price us
doxycycline pills cost
can you buy advair over the counter in mexico
baclofen 20 mg tablet
cialis capsules online
accutane 60 mg
how much is accutane
can you order viagra online in canada
cipro brand name
buy modafinil tablets online
where can you buy azithromycin over the counter
tadacip best price
purchase vermox
advair pill
azithromycin discount drug coupon
can i order cipro online
dexamethasone 10 mg tablet
accutane 40 mg
where can i buy albuterol pills
tadacip 20 mg online
diflucan 150 mg price in india
flomax 0.4 mg capsule
buy zovirax online us
accutane prescription uk
where can i buy furosemide without a script
toradol 70 mg tablet
antibiotic azithromycin
buy sildenafil 20 mg tablets
can you buy retin a over the counter in europe
retin a .1%
where to buy ciprofloxacin
how to get clomid over the counter
buy zithromax online australia
10 mg baclofen pill
order zithromax online
buy accutane pills online
retin a prescription cost
buy 12.5 furosemide online
over the counter clomid
zovirax singapore
effexor 200 mg
lyrica online uk
can i purchase amoxicillin online
diflucan prices
best lasix
lyrica for sale uk
buy lyrica from india
lasix pills for sale
dexamethasone 0 75 mg
strattera prices south africa
tamoxifen price south africa
pharmacy online tadalafil
vermox usa
buy tretinoin 1
buy zithromax uk
can i purchase doxycycline over the counter
buy augmentin online usa
flomax glaucoma
cheap cipro
buy generic accutane
zithromax buy cheap
cipro xr 500
diflucan 150 mg medication
vermox 500mg tablet price
where can i buy vermox
accutane cost in south africa
buying baclofen online
where can i buy vermox tablets
1250 mg prednisone
buy tadacip 20 india
lyrica 100 mg pill
diflucan generic price
furosemide drug
generic tretinoin gel
combivent nebulizer
amoxicillin buy australia
baclofen tablet generic
tretinoin capsules brand name
generic lyrica online
baclofen 10mg tablets
flomax 0.4
geinoutime.com
과거에 이 아들은 무슨 일이 있어도 공부를 열심히 하지 않았습니다.
zithromax 1000mg online
toradol tablet cost
generic advair online
buy clomid online cheap
generic effexor 225 mg
albuterol 63 mg
cipro for sale
how to get tretinoin cream
albuterol without a prescription
viagra pfizer
zithromax 250 g
cipro ciprofloxacin
doxycycline online paypal
modafinil online mexico
accutane 40 mg price
where to purchase doxycycline
propecia mexico
diflucan 1 pill
doxycyline
acyclovir gel
accutane 20 mg price
doxycycline 100mg dogs
ciprofloxacin 5 mg
buy clomid online fast shipping
propecia australia buy
lyrica 250 mg
accutane tablets price
azithromycin capsules 500mg
how to get diflucan
purchase accutane
accutane online india
doxycycline 500 mg capsules
where can you buy diflucan
metformin average cost
how much is tretinoin 1
strattera drug
cipro cost in mexico
can you order valtrex online
lyrica 200 mg capsule
where to get accutane in singapore
order clomid online usa
where to buy nolvadex
azithromycin 500mg price
accutane order
lyrica cost canada
cheap accutane uk
synthroid 0.125 mcg
lasix water pills for sale
generic for combivent
provigil in canada
buy noroxin
dexamethasone for sale
500 mg valtrex daily
provigil 20 mg
propecia in australia
provigil order online canada
azithromycin australia
600 mg zithromax
dexamethasone gel
furosemide 45 mg
lyrica 225 mg
cost prescription acyclovir
sildalis for sale
purchase lasix
buy tadacip online
accutane pills online
propecia pharmacy cost
furosemide 40 mg prices
buy accutane online canada
sildalis without prescription
where to buy metformin 500 mg
how to buy modafinil online uk
where to buy clomid uk
0.05 retin a
dexamethasone 4 mg tablet india
zithromax drug
where to buy albuterol
cheapest generic sildalis
retin a 0.05 cream for sale
zithromax brand name
canadian pharmacy diflucan
vermox 500 tablet
order azithromycin without prescription
azithromycin how to get
amoxicillin 500 mg tablet price
price of generic flomax
can you buy baclofen without a prescription
buy diflucan no prescription
lyrica coupon
lasix 20mg
azithromycin 600 mg price
how to get cialis in australia
where to buy amoxicillin online
baclofen tablets 10mg
zovirax tablets price south africa
clomid 50mg pills
vermox canada
buy doxycycline united states
furosemide 2018
antibiotics zithromax
order furosemide online
synthroid 0.88
accutane tablets uk
albuterol from canada no prescription
baclofen price
online prescription retin a
order lasix 40 mg
cheap accutane
generic lasix online
k8 カジノ パチスロ
この記事の情報は非常に役に立ちます。ありがとうございます。
can you buy accutane in mexico
canadian pharmacy online doxycycline
advair diskus 500 50 mcg coupon
zithromax online pharmacy canada
nolvadex 10 mg tablet
how to get diflucan otc
where can you buy azithromycin over the counter
dexamethasone prescription
toradol 70 mg tablet
amoxicillin 600 mg
ventolin cost usa
geinoutime.com
그러나 당신은 당신이 옳다고 생각합니까, 그렇게 할 수 있습니까?
advair generic
lyrica 50 mg price
modafinil 200mg uk
vermox tablets nz
retin a 1.0 cream prescription
tadacip 20 canada
bactrim f
predisone no rx
price of retin a in mexico
baclofen 75 mg
retin a price in india
order modafinil usa
augmentin 500 coupon
where to buy modafinil online
tamoxifen generic cost
baclofen uk buy
baclofen pills
ventolin for sale uk
combivent average cost
tretinoin cream purchase
baclofen cream price
doxycycline 400 mg price
doxycycline buy online usa
buy propecia canada pharmacy
lasix 3170
where to get female viagra uk
drug lasix 40 mg
where to get synthroid
lasix sale
lyrica 150 mg capsule
카지노 슬롯 머신
마음 속으로 이렇게 말하고 있는 것 같습니다. 폐하, 이렇게 말씀하셨으니 후회하지 마십시오.
propecia buy canada
dexamethasone 0 75 mg
lyrica prescription
advair coupon canada
provigil price canada
buy cheap propecia uk
buy modafinil 200
baclofen cost 10mg
furosemide rx 20 mg
where can i buy metformin tablets
dexamethasone 8 mg
where can i buy albuterol
cheapest lyrica online
how much is a viagra pill cost
zithromax in usa
acyclovir cost australia
order sildenafil online
buy cheap clomid
can i buy nolvadex over the counter
can you buy clomid over the counter in usa
canada pharmacy prednisone
can you buy diflucan over the counter in canada
배팅 룸
다음날 아침 일찍 Fang Jifan은 Xiao Jing이 말한대로 행복하게 궁전에 들어갔습니다.
dexamethasone 0.5
augmentin 875 mg over the counter
토토 캔 배당 분석
Fang Jifan은 감정적으로 말했습니다. “폐하가 돈에 미쳤기 때문일 것입니다.”
buying prescription drugs in mexico: mexican pharmacy – mexican border pharmacies shipping to usa
buy augmentin uk
mexican rx online
https://cmqpharma.com/# medication from mexico pharmacy
mexican drugstore online
acyclovir over the counter canada
albuterol ventolin
flomax cost in india
buy modafinil mexico
where can i get glucophage
lioresal 25 mg
amoxicillin 875 costs
doxycycline price south africa
propecia where to buy uk
where to get modafinil
generic lioresal
tretinoin cream over the counter
buy ciprofloxacin 500mg online
best modafinil brand
accutane generic cost
vibramycin doxycycline
diflucan online prescription
vermox 500 tablet
buy acyclovir australia
tadacip
amoxicillin tablets for sale
zithromax 250 mg tab
generic modafinil online
how to get cipro prescription
propecia cost
metformin singapore pharmacy
buy tadacip online india
buy propecia tablets
ciprofloxacin 500mg antibiotics
strattera 25
lasix 40 mg price in india
baclofen 10 mg pill price
retin a cream price in south africa
buy tadacip canada
acyclovir over the counter australia
cipro no prescription canadian pharmacy
accutane canada pharmacy
where to get ciprofloxacin
cheapest generic tadalafil 20mg
provigil uk prescription
where to purchase viagra online