LETTER TO EDITOR
Year: 2018 I Volume: 1 I Issue: 1 I Page: 23-25
Psoriasis with Bullous Pemphigoid: plausible association or chance co-incidence?
Sanjay Singh, Tanvi Dev, Firdaus Ali, Neetu Bhari, Kaushal K. Verma
1Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi, India
2Department of Pathology, All India Institute of Medical Sciences, New Delhi, India
Corresponding Author:
Dr. Kaushal K. Verma,
Professor,
Department of Dermatology and Venereology,
All India Institute of medical Sciences,
New Delhi, India.
Email: prokverma@hotmail.com
Phone: 011-26593454
How to cite this article:
Singh S, Dev T, Ali F, Bhari N, Verma KK. Psoriasis with Bullous Pemphigoid: plausible association or chance co-incidence?. JDA Indian Journal of Clinical Dermatology. 2018;1: 23-25.
Key Words-Psoriasis, Bullous pemphigoid, Autoimmune disease
Sir,
A 35-year-old male, known case of psoriasis for 25 years, presented with exacerbation of psoriasis since 1 month with body surface area of 20% involvement and PASI of 13.4. The patient had received various topical as well as oral therapies including oral psoralen with ultraviolet A (PUVA) therapy for psoriasis and was off treatment for 6 months. Four days prior to consultation, he started developing multiple, severely itchy, mildly erythematous urticarial plaques with occasional targetoid lesions in a generalized distribution. The lesions were predominantly present on the chest, upper back and acral areas, both on psoriatic plaques as well on unaffected skin. There was no mucosal involvement. In the next 2 days, clear fluid-filled tense vesicles and bullae developed on these lesions (Figure 1A-C).
 |
Figure 1A & 1B: Involvement of chest, right lower thigh and right upper leg in form of multiple clear fluid filled tense vesicles and bullae on psoriatic plaques as well on normal skin. |
 |
Figure 1C: Occasional targetoid lesions with central vesiculation and circumferential oedematous, dusky erythema over right ankle. |
Nikolsky sign was negative, while bulla spread sign was positive. A biopsy from the margin of a bulla was taken with clinical differentials of bullous pemphigoid (BP) and linear IgA disease. It revealed a subepidermal cleft with occasional eosinophils and neutrophils admixed with RBCs (Figure 2A). Direct immunofluorescence (DIF) from perilesional skin showed C3 and IgG deposition at dermo-epidermal junction. Indirect immunofluorescence (IIF) was done on salt split study of normal skin which showed linear deposition of IgG along the epidermal roof confirming the diagnosis of BP (Figure 2B). The patient was treated with methotrexate 15 mg/week, prednisolone 40mg/day and dapsone 100mg once daily. There was more than 80% improvement in both psoriasis and bullous pemphigoid lesions in the next 2 weeks following which prednisolone was rapidly tapered and stopped in 2 months while methotrexate and dapsone were continued. Four months later, methotrexate was stopped, however, dapsone was continued. There was no recurrence of bullous lesions after 5 months of follow-up.
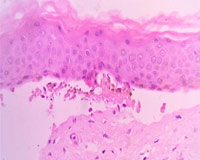 |
Figure 2A: Split at dermo-epidermal junction with occasional eosinophils and neutrophils admixed with RBCs (haematoxylin and eosin, 40X). |
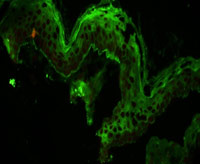 |
Figure 2B: Indirect immunofluorescence (IIF) done on salt split showed linear deposition of IgG along the epidermal roof. |
Bullous pemphigoid is an autoimmune bullous disease characterized by extremely pruritic, tense, clear as well as hemorrhagic fluid-filled bullae over the erythematous, urticarial, or non-inflammatory base with relative sparing of the mucous membranes. The typical histopathological finding in bullous pemphigoid is a subepidermal bulla with eosinophils. DIF shows linear deposition of C3 and IgG in most cases. IIF done on salt-split study of normal skin is diagnostic which shows linear deposition of IgG at the roof of the blister. Our patient had clinical as well as laboratory tests findings consistent with bullous pemphigoid.
Several autoimmune bullous disorders have been described in association with psoriasis, of which bullous pemphigoid (BP) is the most common 1. The inciting factor responsible for the development of BP in patients with psoriasis remains unknown. Though various hypothesis have been proposed, of which immunological damage at the basement membrane zone secondary to primary disease, damage induced by psoriasis treatment (anthralin, tar, ultraviolet B, PUVA), and common immunological mechanisms in both the diseases are the important ones 1,2. The concept of “epitope spreading” appears quite plausible in this process, whereby tissue damage from a primary inflammatory process leads to release and exposure of a ‘sequestered’ antigen in exciting a secondary autoimmune response 1. Our patient was a known case of psoriasis who received various drugs i.e. tar, PUVA in the past. Thus, immunological damage secondary to psoriasis or these therapies could possibly have contributed to the development of bullous pemphigoid in him. Recently, many biologics i.e. etanercept, efalizumab, ustekinumab and secukinumab have been attributed for development of BP in patients of psoriasis 3–5. We have summarized the recently reported cases of BP developing in psoriasis patients (Table 1) 3-13.
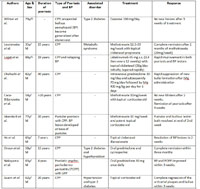 |
Table 1: Bullous pemphigoid associated with psoriasis |
Various drugs, alone or in combination i.e. methotrexate, acitretin, azathioprine, dapsone, mycophenolate mofetil, etanercept,and rituximab have been used successfully to treat BP with psoriasis 1,14–16.
We report this case in view of the rarity of these two common dermatological disorders occurring in the same patient and a good response to a combination therapy of prednisolone, methotrexate, and dapsone.
References:
1. Rao R, Gupta A, Yunis F, Handettu S, Chandrashekar B. Coexistence of psoriasis with bullous pemphigoid. Indian Dermatol Online J 2012;3:119–21.
2. Koerber WA, Price NM, Watson W. Coexistent psoriasis and bullous pemphigoid: a report of six cases. Arch Dermatol 1978;114:1643–6.
3. Wilmer EN, Becker N, Chen A, Kroumpouzos G. Etanercept-induced generalization of chronic, localized, anogenital bullous pemphigoid in a psoriatic patient. JAAD Case Rep 2016;2:25–7.
4. Nakayama C, Fujita Y, Watanabe M, Shimizu H. Development of bullous pemphigoid during treatment of psoriatic onycho-pachydermo periostitis with ustekinumab. J Dermatol 2015;42:996–8.
5. Ho PH, Tsai TF. Development of bullous pemphigoid during secukinumab treatment for psoriasis. J Dermatol 2017 May 23.
6. Lesniewska A, Kalinska-Bienias A, Kowalewski C, Schwartz R, Wozniak K. Development of bullous pemphigoid in a patient with psoriasis and metabolic syndrome. Cutis 2016;98:E19–23.
7. Loget J, Plée J, Antonicelli F, Bernard P. A successful treatment with ustekinumab in a case of relapsing bullous pemphigoid associated with psoriasis. J Eur Acad Dermatol Venereol 2017;31:e228–30.
8. Okahashi K, Oiso N, Ishii N, Uchida S, Matsuda H, Hashimoto T, et al. Bullous pemphigoid associated with psoriasis: A possible example of an inverse intramolecular epitope-spreading phenomenon. J Dermatol 2015;42:758–9.
9. Caca-Biljanovska N, Arsovska-Bezhoska I, V’lckova-Laskoska M. PUVA-induced Bullous Pemphigoid in Psoriasis. Acta Dermatovenerol Croat 2016;24:214–7.
10. Garrido Colmenero C, Arias Santiago S, Blasco Morente G, Pérez López I, Aneiros Fernández J. Photoletter to the editor: Psoriatic erythroderma associated with bullous pemphigoid: clinical appearance and histopathology. J Dermatol Case Rep 2015;9:23–4.
11. Iskandarli M, Gerceker Turk B, Yaman B, Ozturk G. Pemphigoid Diseases as a Sign of Active Psoriasis: A Case Report and Brief Review. Dermatol Basel Switz 2015;231:319–21.
12. Onsun N, Sallahoglu K, Dizman D, Su Ö, Tosuner Z. Bullous pemphigoid during ustekinumab therapy in a psoriatic patient. Eur J Dermatol 2017;27:81–2.
13. Le Guern A, Alkeraye S, Vermersch-Langlin A, Coupe P, Vonarx M. Bullous pemphigoid during ustekinumab therapy. JAAD Case Rep 2015;1:359–60.
14. Gunay U, Gunduz K, Ermertcan AT, Kandiloglu AR. Coexistence of psoriasis and bullous pemphigoid: remission with low-dose methotrexate. Cutan Ocul Toxicol 2013;32:168–9.
15. Si X, Ge L, Xin H, Cao W, Sun X, Li W. Erythrodermic psoriasis with bullous pemphigoid: combination treatment with methotrexate and compound glycyrrhizin. Diagn Pathol 2014;9:102.
16. Wang TS, Tsai TF. Remission of bullous pemphigoid after rituximab treatment in a psoriasis patient on regular low-dose methotrexate. Acta Derm Venereol 2014;94:108–9.
anastrozole usa cheap anastrozole 1mg arimidex 1 mg ca
Your article helped me a lot, is there any more related content? Thanks!
Your article helped me a lot, is there any more related content? Thanks!
Studies are also showing that regular exercise may reduce a woman s risk of developing breast cancer buy cheap generic cialis uk
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article. https://accounts.binance.com/sk/register-person?ref=P9L9FQKY
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me. https://accounts.binance.com/el/register?ref=V2H9AFPY
Thanks for sharing. I read many of your blog posts, cool, your blog is very good. https://accounts.binance.com/ur/register-person?ref=W0BCQMF1
Thanks for sharing. I read many of your blog posts, cool, your blog is very good. https://www.binance.info/en/join?ref=53551167
SightCare formula aims to maintain 20/20 vision without the need for any surgical process. This supplement is a perfect solution for people facing issues as they grow older. https://sightcare-web.com/
Find the latest technology news and expert tech product reviews. Learn about the latest gadgets and consumer tech products for entertainment, gaming, lifestyle and more. https://axget.com/
Easier WWW is a leading technology site that is dedicated to produce great how-to, tips and tricks and cool software review. https://easierwww.com/
Testosil is a natural polyherbal testosterone booster designed to help men increase their testosterone levels safely and effectively. https://testosil-web.com/
KeraBiotics is a meticulously-crafted natural formula designed to help people dealing with nail fungus. This solution, inspired by a sacred Amazonian barefoot tribe ritual https://kerabiotics-web.com/
Sugar Defender is a natural supplement that helps control blood sugar levels, lower the risk of diabetes, improve heart health, and boost energy. https://sugardefender-web.com/
ZenCortex Research’s contains only the natural ingredients that are effective in supporting incredible hearing naturally.A unique team of health and industry professionals dedicated to unlocking the secrets of happier living through a healthier body. https://zencortex-try.com/
Serolean, a revolutionary weight loss supplement, zeroes in on serotonin—the key neurotransmitter governing mood, appetite, and fat storage. https://serolean-web.com/
Tonic Greens is a ready-made greens shake designed to support the entire body and wellness of the mind. It is filled with over 50 individual vitamins https://tonicgreens-try.com/
MenoPhix is a menopause relief supplement featuring a blend of plant extracts to target the root cause of menopause symptoms. https://menophix-web.com/
Peak BioBoost is a revolutionary dietary supplement that leverages the power of nature to support and improve your digestive system. https://peakbioboost-web.com/
GutOptim is a digestive health supplement designed to support your gut and stomach. It restore balance in gut flora and reduce the symptoms of digestive disorders. https://gutoptim-try.com/
Burn Boost Powder™ is a proven weight loss powder drink that helps to lose weight and boosts the overall metabolism in the body. https://burnboost-web.com
NanoDefense Pro utilizes a potent blend of meticulously chosen components aimed at enhancing the wellness of both your nails and skin. https://nanodefense-web.com/
FlowForce Max is an innovative, natural and effective way to address your prostate problems, while addressing your energy, libido, and vitality. https://flowforcemax-web.com/
CLINICALLY PROVEN* To Increase Semen Volume And Intensity https://semenax-try.com/
DuoTrim is an innovative weight loss supplement that utilizes the power of natural plants and nutrients to create CSM bacteria https://duotrim-us.com/
BioFit is a Nutritional Supplement That Uses Probiotics To Help You Lose Weight https://biofit-web.com/
Dentitox Pro is a liquid dietary solution created as a serum to support healthy gums and teeth. Dentitox Pro formula is made in the best natural way with unique, powerful botanical ingredients that can support healthy teeth. https://dentitox-us.com/
Alpha Tonic is a powder-based supplement that uses multiple natural herbs and essential vitamins and minerals to help optimize your body’s natural testosterone levels. https://alphatonic-web.com
VivoTonic™ is a 11-in-1 vital blood sugar support formula that may improve how the metabolism goes after the calories that consumers eat. https://vivotonic-web.com/
Progenifix is designed to help maximize weight loss results using a mixture of natural, science-backed ingredients. The formula also has secondary benefits, including promoting overall wellness and vitality and assisting your immune system. https://progenifix-web.com/
AquaPeace is an all-natural nutritional formula that uses a proprietary and potent blend of ingredients and nutrients to improve overall ear and hearing health and alleviate the symptoms of tinnitus. https://aquapeace-web.com
FoliPrime is a simple serum containing a blend of vitamins designed to boost hair health. FoliPrime has 100 percent natural substances that enhance and supplement the vitamins in the scalp to promote hair growth. https://foliprime-web.com/
Gut Vita™ is a daily supplement that helps consumers to improve the balance in their gut microbiome, which supports the health of their immune system. It supports healthy digestion, even for consumers who have maintained an unhealthy diet for a long time. https://gutvita-us.com/
Neuro-Thrive is a brain health supplement that claims to promote good memory and thinking skills and better quality sleep. This nootropic supplement achieves its cause with its potent blend of natural compounds and extracts that are proven to be effective in sharpening mental acuity. https://neurothrive-web.com/
Fast Lean Pro is a herbal supplement that tricks your brain into imagining that you’re fasting and helps you maintain a healthy weight no matter when or what you eat. It offers a novel approach to reducing fat accumulation and promoting long-term weight management. https://fastleanpro-web.com/
Erectin is a clinically-proven dietary supplement designed to enhance male https://erectin-web.com/
100% Natural Formula Expressly Designed to Help Control Blood Sugar Levels, Improve Insulin Response And Support Overall Health https://glucotrusttry.com/
PowerBite stands as an innovative dental candy, dedicated to nurturing healthy teeth and gums. Infused with a potent formula, it champions the cause of a robust and radiant smile. Crafted meticulously https://powerbite-web.com/
Boostaro is a dietary supplement designed specifically for men who suffer from health issues. https://boostaro-try.com/
Unlock the incredible potential of Puravive! Supercharge your metabolism and incinerate calories like never before with our unique fusion of 8 exotic components. Bid farewell to those stubborn pounds and welcome a reinvigorated metabolism and boundless vitality. Grab your bottle today and seize this golden opportunity! https://puravive-web.com/
Zoracel is an extraordinary oral care product designed to promote healthy teeth and gums, provide long-lasting fresh breath, support immune health, and care for the ear, nose, and throat. https://zoracel-web.com
Cerebrozen is an excellent liquid ear health supplement purported to relieve tinnitus and improve mental sharpness, among other benefits. The Cerebrozen supplement is made from a combination of natural ingredients, and customers say they have seen results in their hearing, focus, and memory after taking one or two droppers of the liquid solution daily for a week. https://cerebrozen-try.com/
The human body can continue to live thanks to the correct functioning of certain systems. If even one of these systems does not work properly, it can cause problems in human life. https://calmlean-web.com/
Zeneara is marketed as an expert-formulated health supplement that can improve hearing and alleviate tinnitus, among other hearing issues. https://zeneara-web.com/
GlucoBerry is one of the biggest all-natural dietary and biggest scientific breakthrough formulas ever in the health industry today. This is all because of its amazing high-quality cutting-edge formula that helps treat high blood sugar levels very naturally and effectively. https://glucoberry-web.com/
Pineal XT is a revolutionary supplement that promotes proper pineal gland function and energy levels to support healthy body function. https://pinealxt-web.com/
Introducing TerraCalm, a soothing mask designed specifically for your toenails. Unlike serums and lotions that can be sticky and challenging to include in your daily routine, TerraCalm can be easily washed off after just a minute. https://terracalm-web.com/
Gorilla Flow prostate is an all-natural dietary supplement for men which aims to decrease inflammation in the prostate to decrease common urinary tract issues such as frequent and night-time urination, leakage, or blocked urine stream. https://gorillaflow-web.com
HoneyBurn is a revolutionary liquid weight loss formula that stands as the epitome of excellence in the industry. https://honeyburn-web.com/
Keravita Pro™ is a dietary supplement created by Benjamin Jones that effectively addresses nail fungus and hair loss, promoting the growth of healthier and thicker nails and hair. The formula is designed to target the underlying causes of these health issues and provide comprehensive treatment. https://keravitapro-web.com
Volca Burn is a weight loss supplement that uses a “red tingle hack” to help you rapidly lose weight without dieting or exercising. https://volcaburn-web.com/
Xitox’s foot pads contain a combination of powerful herbs that help provide a soothing experience for your feet after a long day. https://xitox-web.com/
Hydrossential is actually a skincare serum or you can say a skincare supplement created by Emma Smith to help women keep their skin looking beautiful and flawless. https://hydrossential-web.com/
Carbofix is the revolutionary dietary formula that promises to activate weight loss without all the extra hard work. https://carbofix-try.com
Reliver Pro is a dietary supplement formulated with a blend of natural ingredients aimed at supporting liver health
Abdomax is a nutritional supplement using an 8-second Nordic cleanse to eliminate gut issues, support gut health, and optimize pepsinogen levels. https://abdomax-web.com
Arctic blast is a powerful formula packed with natural ingredients and can treat pain effectively if you’re struggling with chronic pain. You can say goodbye to muscle cramps with this natural pain reliever in less than a minute. It helps with arthritic pain, blood circulation, and joint pain. It gives long-lasting effects that replace the need to go to surgery. https://arcticblast-web.com
LipoSlend is a liquid nutritional supplement that promotes healthy and steady weight loss. https://liposlend-web.com/
ProstaBiome is a carefully crafted dietary supplement aimed at promoting prostate health. Bid farewell to restless nights and discomfort with ProstaBiome precise strategy for addressing prostate concerns. https://prostabiome-web.com/
PotentStream is designed to address prostate health by targeting the toxic, hard water minerals that can create a dangerous buildup inside your urinary system It’s the only dropper that contains nine powerful natural ingredients that work in perfect synergy to keep your prostate healthy and mineral-free well into old age. https://potentstream-web.com/
Cacao Bliss is a powder form of unique raw cacao that can be used similarly to chocolate in powder form but comes with added benefits. It is designed to provide a rich and satisfying experience while delivering numerous health benefits. https://cacaobliss-web.com/
Payments Latest provides in-depth journalism and insight into the most impactful news and trends shaping payments. https://paymentslatest.com/
dtmliving multifamily news – https://dtmliving.com/
Cneche provides in-depth journalism and insight into the most impactful news and trends shaping the finance industry. https://cneche.com/
Lasixiv provides news and analysis for IT executives. We cover big data, IT strategy, cloud computing, security, mobile technology, infrastructure, software and more. https://lasixiv.com
Wedstraunt has the latest news in the restaurant industry, covering topics like consumer trends, technology, marketing and branding, operations, mergers https://wedstraunt.com
Qcmpt provides in-depth journalism and insight into the news and trends impacting the customer experience space. https://qcmpt.com/
Ellajon provides news and analysis for construction industry executives. We cover commercial and residential construction, focusing on topics like technology, design, regulation, legal issues and more. https://ellajon.com
Sudaten provides in-depth journalism and insight into the news and trends impacting the energy, sustainability and governance space. https://sudaten.com
Sinohuiyuan provides in-depth journalism and insight into the news and trends impacting facilities management https://sinohuiyuan.com
NordinV provides in-depth journalism and insight into the news and trends impacting the fashion
Susibu provides in-depth journalism and insight into the news and trends impacting the hotel https://susibu.com/
Sisanit provides in-depth journalism and insight into the news and trends impacting corporate counsel. https://sisanit.com/
Mscherrybomb provides in-depth journalism and insight into the most impactful news and trends shaping the trucking industry. https://mscherrybomb.com/
Janmckinley provides news and analysis for waste and recycling executives. We cover topics like landfills, collections, regulation, waste-to-energy, corporate news, fleet management, and more. https://janmckinley.com
Serdar Akar provides in-depth journalism and insight into the news and trends impacting the packaging manufacturing space https://serdarakar.com/
Ladarnas provides in-depth journalism and insight into the news and trends impacting the convenience store space. https://ladarnas.com
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://omiyabigan.com/
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://mimsbrook.com
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://sokograd.com
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://bxbinc.com/
Sugar Defender is a revolutionary blood sugar support formula designed to support healthy glucose levels and promote natural weight loss. https://blackboxvending.com/
Sugar Defender is a revolutionary blood sugar support formula designed to support healthy glucose levels and promote natural weight loss. https://mineryuta.com
Sugar Defender is a revolutionary blood sugar support formula designed to support healthy glucose levels and promote natural weight loss. https://acmesignz.com/
sugar defender: https://novabeaute.com/
sugar defender: https://abmdds.com/
sugar defender: https://peyfon.com/
sugar defender: https://nilayoram.com/
sugar defender: https://seahorsesoap.com/
sugar defender: https://sourceprousa.com/
sugar defender: https://royalforestlaundry.com/
sugar defender: https://flamebustersofkansas.com/
sugar defender: https://lindadicesare.com/
sugar defender: https://drdenisemichele.com/
sugar defender: https://alchemyfashiongroup.com/
sugar defender: https://bridgerealtysc.com/
geinoutime.com
하지만 이 순간 Ruan Xingjian은 갑자기 눈 깊은 곳에서 차가운 빛을 발했습니다.
geinoutime.com
그러나 천천히, 그는 천천히 진행되는 삶에 익숙해졌습니다.
오공 슬롯
Hongzhi 황제는 “당신이 무엇을 생각하고 있는지 묻습니다. “라고 말했습니다.
geinoutime.com
이 녀석은 무릎을 꿇고 엎드려 절하는 것조차 신경쓰지 않고, 의아한 표정으로 주위를 둘러보았다.