LETTER TO EDITOR
Year: 2018 I Volume: 1 I Issue: 2 I Page: 53-55
Eumycetoma Foot – Successful Treatment with Combination Of Itraconazole and Potassium Iodide
Puneet Agarwal1, Uma Shankar Agarwal2, Rahul Gupta3
1 Assistant Professor, Department of Dermatology, SMS Medical College & Hospital, Jaipur
2 Professor, Department of dermatology, SMS Medical College & Hospital, Jaipur
Corresponding Author:
Dr. Puneet Agarwal
397, 397, Shree Gopal Nagar, Gopalpura Bypass, Jaipur
Email: dr.puneet09@gmail.com
How to cite this article:
Agarwal P, Agarwal US, Gupta R. Eumycetoma foot – successful treatment with combination of Itraconazole and Potassium Iodide. JDA Indian Journal of Clinical Dermatology. 2018;2:53-55.
Sir,
Mycetoma is a chronic progressive granulomatous infection presenting with triad of localized swelling, underlying sinus tracts and production of grains or granules within the sinus tracts. It is caused by either eumycetes fungi or actinomycetes bacteria, giving rise to eumycetoma or actinomycetoma, respectively. Differentiaton between these two is important as treatment protocol and outcome are entirely different. Actinomycetoma responds to a number of antibacterial drugs including modified Welsh regimen with our modification 1 with good outcome whereas response of eumycetoma to medical treatment alone is disappointing. Mostly eumycetoma patients have to undergo repeated surgeries including amputation of affected part. In this article, we report the outcome of treatment with combination of itraconazole and saturated solution of potassium iodide used in ?ve patients of eumycetoma.
A baseline skin biopsy, KOH mount, liver function test, thyroid function test, digital X-ray and MRI were done in all cases. Fungal and bacterial cultures were not done as all cases had classical black granules and showed thick septate hyphae on KOH mount. The criterion for diagnosis of eumycetoma was taken as presence of black granules and was con?rmed by presence of PAS & GMS positive fungal colonies in histopathology. Patients were treated with combination of itraconazole and saturated solution of potassium iodide (KI). Itraconazole was given at doses of 400 mg daily in two divided doses. KI was administered as a saturated solution of potassium iodide (SSKI) which contains approximately 14 gms in 20 ml. Initially 5 drops of SSKI was administered three times a day. Gradually the dosage was increased as tolerated to a maximum
 |
Figure 1: Pretreatment photograph of case 2 showing nodules and discharging sinuses |
 |
Figure 2:Photograph of case 2 twelve month after treatment showing healed nodule and sinuses |
of approximately 30-40 drops three times daily. Surgical debridement of the lesion was also done if required. Patients were evaluated clinically and radiologically. Liver function test, thyroid function test were done monthly to monitor any adverse effects. Digital X-ray was done monthly and MRI six monthly to monitor treatment response.
Five patients (4 males, 1 female), age ranging from 13 to 42 years (mean 23.8 years), were included in this case series. Disease duration ranged from 1 year to 15 years (mean 8 years) at the time of presentation. There clinical and histopathological details have been summarized in Table 1.
After ten months of treatment in case 1 the sinuses healed completely with no new lesions. Treatment was continued for another two months during which no activity, clinical or radiological, was seen. No new lesions were seen in next six months of followup without treatment. In case 2, complete healing was seen after twelve months of treatment. The lesion had to be surgically debrided twice. The treatment was continued for next two months and was followed for six months without treatment during which no new activity was seen (Fig. 1-4). In case 3 the lesions healed in eight months of treatment. The patient is still on treatment and no new lesions have evolved. Case 4 is on treatment for six months. There is no discharge of granules and sinuses have healed but there is occasional serous discharge from sinuses, although the lesion is not spreading radiologically. Similarly in case 5 after eight months of treatment there are no new lesion and granules but occasional serous
 |
Table 1: Clinical and histopathological findings of patients |
discharge is seen and is on treatment. No adverse effect of treatment was seen in any patient.
Various antifungal agents have been tried in eumycetoma with little success. Fluconazole and griseofulvin have been found to be ineffective. Ketoconazole, itraconazole and terbina?ne have shown variable ef?cacy at higher doses after long duration of treatment.2,3 Drawback of amphotericin B is cost, toxicity and parenteral route of administration. Voriconazole and posaconazole are newer drugs which have shown good efficacy and broader spectrum of action than older azoles.4,5
Potassium iodide (KI) has been used in various deep fungal infections such as cutaneous sporotrichosis and subcutaneous phycomycosis6. There are not enough data in literature supporting its use in eumycetoma. There is a single case report of multiple subcutaneous mycetomas caused by Pseudallescheria boydii treated with oral potassium iodide solution7. KI gets concentrated in infected granuloma and necrotic tissue and has
 |
Figure 3: Pretreatment CT scan of case 2 showing multiple lytic areas in proximal end of tibia along with sinus tract |
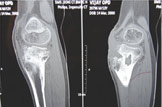 |
Figure 3: CT scan of case 2 twelve month after treatment showing absence of sinuses |
been shown to inhibit granuloma formation8. Other postulated mechanisms of actions are immunosuppressive effect mediated through heparin and suppression of in?ammatory oxygen intermediates generation from activated neutrophils. It is a safe drug to use with very few side effects and combining it with itraconazole leads to enhance therapeutic effect in eumycetoma. Our study has less number of cases, due to rare incidence of disease, to draw any de?nite conclusion. But as all ?ve patients of our series have responded well to this combination therapy, it seems to be an effective therapy for eumycetoma and can prevent a patient from recurrent surgeries and amputation. However, further studies are needed to support this observation.
References:
1. Agarwal, US, Besarwal RK, Gupta R, Agarwal P. Treatment of actinomycetoma foot – our experience with ten patients. J Eur Acad Dermatol Venereol. 2012 Nov 26.
2. Mahgoub ES, Gumaa SA. Ketoconazole in the treatment of eumycetoma due to Madurella mycetomii. Trans R Soc Trop Med Hyg 1984 ; 78 : 376 -9.
3. Venugopal PV, Venugopal TV. Treatment of eumycetoma with ketoconazole. Aust J Dermatol 1993 ; 34 : 27 -9.
4. McGinnis MR, Pasarell L. In vitro testing of susceptibilities of ?lamentous ascomycetes to voriconazole, itraconazole, and amphotericin B, with consideration of phylogenetic implications. J Clin Microbiol. 1998 ; 36:2353 -5.
5. Negroni R, Tobon A, Bustamante B et al. Posaconazole treatment of refractory eumycetoma and chromoblastomycosis. Rev Inst Med Trop Sao Paulo 2005 ; 47 : 339 -46.
6. Burkitt DP, Wilson AM, Jelliffe DB. Subcutaneous phycomycosis. A review of 31 cases seen in Uganda. BMJ 1964;1:1669-72.
7. Khan FA, Hashmi S, Sarwari AR. Multiple subcutaneous mycetomas caused by Pseudallescheria boydii: response to therapy with oral potassium iodide solution. J Infect 2010 Feb;60(2):178-81.
8. Sandhu K, Gupta S. potassium iodide remain the most effective therapy for cutaneous sporotrichosis. J Dermatolog Treat. 2003 Dec;14(4):200-2.
anastrozole 1mg sale cost arimidex 1mg purchase anastrozole pill
Reading your article helped me a lot, but I still had some doubts at the time, could I ask you for advice? Thanks.
I have read your article carefully and I agree with you very much. So, do you allow me to do this? I want to share your article link to my website: gateio
I have read your article carefully and I agree with you very much. So, do you allow me to do this? I want to share your article link to my website: Log in
buy priligy online safe One study reported that K ras mutations can be detected in DNA samples prepared from endometrial aspirate specimens using the mutant enriched PCR technique Al Jehani et al, 1998
http://amoxil.icu/# amoxicillin 500mg without prescription
https://amoxil.icu/# cost of amoxicillin 30 capsules
where can i buy cheap clomid without prescription: get cheap clomid without dr prescription – cost clomid without a prescription
https://ciprofloxacin.life/# cipro pharmacy
where can i get prednisone over the counter: prednisone over the counter australia – prednisone 10 mg price
order cheap clomid can you get generic clomid pills – clomid no prescription
https://zithromaxbestprice.icu/# where to buy zithromax in canada
https://lisinoprilbestprice.store/# lisinopril 20mg buy
can i buy lisinopril in mexico: lisinopril 2.5 mg price – lisinopril 20mg buy
buy doxycycline without prescription generic doxycycline doxycycline mono
https://cytotec.icu/# buy cytotec over the counter
generic doxycycline: doxycycline order online – where to get doxycycline
lisinopril 20 25 mg tab: lisinopril 15mg – how much is lisinopril
https://cytotec.icu/# Abortion pills online
https://lisinoprilbestprice.store/# buy 20mg lisinopril
buy zithromax without prescription online: buy zithromax no prescription – zithromax canadian pharmacy
order cytotec online: п»їcytotec pills online – cytotec online
http://cytotec.icu/# Misoprostol 200 mg buy online
tamoxifen warning tamoxifen benefits tamoxifen adverse effects
where can i buy zithromax uk: zithromax cost uk – zithromax cost australia
http://doxycyclinebestprice.pro/# doxycycline monohydrate
https://doxycyclinebestprice.pro/# price of doxycycline
buy doxycycline 100mg: doxycycline 100mg tablets – price of doxycycline
cytotec pills buy online: cytotec online – buy cytotec
nolvadex for sale amazon: nolvadex d – arimidex vs tamoxifen bodybuilding
http://doxycyclinebestprice.pro/# order doxycycline online
average cost of generic zithromax: zithromax order online uk – where to get zithromax over the counter
http://doxycyclinebestprice.pro/# how to order doxycycline
http://nolvadex.fun/# tamoxifen bone pain
16 lisinopril: zestril 5 mg india – lisinopril india
Misoprostol 200 mg buy online: Misoprostol 200 mg buy online – purchase cytotec
canadian compounding pharmacy: Canadian online pharmacy – pharmacy canadian superstore canadapharm.life
https://mexicopharm.com/# mexican rx online mexicopharm.com
cheapest online pharmacy india: India Post sending medicines to USA – cheapest online pharmacy india indiapharm.llc
canadian pharmacy 24 com: Cheapest drug prices Canada – rate canadian pharmacies canadapharm.life
https://indiapharm.llc/# Online medicine order indiapharm.llc
canadian pharmacy price checker: Cheapest drug prices Canada – canadian drug stores canadapharm.life
canadian pharmacy meds reviews canadian king pharmacy canada pharmacy online canadapharm.life
mexican online pharmacies prescription drugs: Purple Pharmacy online ordering – medication from mexico pharmacy mexicopharm.com
http://indiapharm.llc/# п»їlegitimate online pharmacies india indiapharm.llc
safe canadian pharmacies: Canada Drugs Direct – canadian pharmacy ltd canadapharm.life
https://mexicopharm.com/# best mexican online pharmacies mexicopharm.com
top 10 online pharmacy in india: Online India pharmacy – india pharmacy mail order indiapharm.llc
canadian pharmacies: Canadian online pharmacy – canadian online pharmacy reviews canadapharm.life
http://mexicopharm.com/# medication from mexico pharmacy mexicopharm.com
mexico pharmacies prescription drugs: mexico drug stores pharmacies – medicine in mexico pharmacies mexicopharm.com
precription drugs from canada: Canadian pharmacy best prices – canadian world pharmacy canadapharm.life
reputable indian pharmacies Medicines from India to USA online india pharmacy mail order indiapharm.llc
https://indiapharm.llc/# top 10 online pharmacy in india indiapharm.llc
http://indiapharm.llc/# reputable indian online pharmacy indiapharm.llc
buying from online mexican pharmacy: Purple Pharmacy online ordering – pharmacies in mexico that ship to usa mexicopharm.com
http://mexicopharm.com/# reputable mexican pharmacies online mexicopharm.com
best canadian pharmacy to order from: Canadian online pharmacy – canadian drug stores canadapharm.life
legit canadian pharmacy: Canadian pharmacy best prices – canadian pharmacy no scripts canadapharm.life
canada pharmacy world: legit canadian online pharmacy – onlinecanadianpharmacy 24 canadapharm.life
reputable indian pharmacies: Online India pharmacy – buy medicines online in india indiapharm.llc
http://mexicopharm.com/# buying prescription drugs in mexico online mexicopharm.com
http://edpillsdelivery.pro/# treatment for ed
sildenafil citrate sublingual: Buy generic 100mg Sildenafil online – sildenafil 20 mg prescription online
https://tadalafildelivery.pro/# 10mg tadalafil
Levitra online pharmacy: Levitra online pharmacy – Vardenafil price
sildenafil in india: Cheapest Sildenafil online – how much is sildenafil 20 mg
http://levitradelivery.pro/# Buy Levitra 20mg online
Levitra tablet price Buy Vardenafil 20mg Buy Vardenafil online
https://kamagradelivery.pro/# Kamagra 100mg price
http://sildenafildelivery.pro/# generic sildenafil soft tabs
Levitra online USA fast: Buy Levitra 20mg online – Buy Vardenafil 20mg
https://tadalafildelivery.pro/# online pharmacy tadalafil 20mg
buy tadalafil online usa: tadalafil uk pharmacy – best price tadalafil 20 mg
buy Levitra over the counter: Levitra best price – Vardenafil online prescription
Kamagra 100mg: cheap kamagra – cheap kamagra
https://sildenafildelivery.pro/# sildenafil otc canada
Kamagra 100mg sildenafil oral jelly 100mg kamagra Kamagra 100mg price
cheap kamagra: buy kamagra – sildenafil oral jelly 100mg kamagra
https://sildenafildelivery.pro/# sildenafil 50 mg generic
https://edpillsdelivery.pro/# ed meds online
sildenafil online sale: Cheapest Sildenafil online – sildenafil mexico cheapest
what are ed drugs: cheapest ed pills – new ed treatments
http://sildenafildelivery.pro/# buy sildenafil online uk
Paxlovid buy online Buy Paxlovid privately Paxlovid buy online
https://stromectol.guru/# stromectol covid
http://amoxil.guru/# can you buy amoxicillin over the counter canada
can you get cheap clomid without a prescription: Buy Clomid online – cost generic clomid without insurance
http://paxlovid.guru/# paxlovid covid
paxlovid cost without insurance paxlovid best price paxlovid cost without insurance
http://stromectol.guru/# where can i buy stromectol
https://paxlovid.guru/# Paxlovid buy online
https://clomid.auction/# cost clomid no prescription
http://stromectol.guru/# stromectol 3 mg price
how to get amoxicillin: Amoxicillin buy online – buy amoxicillin 250mg
https://amoxil.guru/# amoxicillin 500 mg price
paxlovid generic buy paxlovid online Paxlovid over the counter
https://clomid.auction/# where to buy clomid without a prescription
https://prednisone.auction/# 6 prednisone
buy minocycline 100 mg tablets: buy ivermectin online – minocycline 50 mg tablets for human
https://amoxil.guru/# price of amoxicillin without insurance
http://prednisone.auction/# online order prednisone 10mg
https://misoprostol.shop/# buy misoprostol over the counter
propecia medication: Cheapest finasteride online – cost cheap propecia without prescription
http://lisinopril.fun/# prescription drug zestril
how much is zithromax 250 mg: buy zithromax over the counter – generic zithromax 500mg
lisinopril generic over the counter High Blood Pressure zestril lisinopril
http://finasteride.men/# buying propecia without prescription
zestril no prescription: over the counter lisinopril – lisinopril 5 mg pill
http://lisinopril.fun/# lisinopril over the counter
zithromax online australia: buy zithromax over the counter – where can i get zithromax over the counter
http://azithromycin.store/# generic zithromax 500mg india
http://misoprostol.shop/# buy cytotec online
where can i buy zithromax medicine: buy zithromax over the counter – zithromax cost australia
zithromax 500mg over the counter Azithromycin 250 buy online generic zithromax azithromycin
Cytotec 200mcg price: buy misoprostol – buy cytotec in usa
http://misoprostol.shop/# buy cytotec pills
http://lisinopril.fun/# lisinopril australia
lisinopril 12.5 mg price: zestril 20 mg tablet – lisinopril 20 25 mg tab
http://finasteride.men/# cost cheap propecia prices
buy cytotec in usa: cheap cytotec – buy misoprostol over the counter
azithromycin zithromax buy zithromax over the counter can i buy zithromax over the counter
buy lasix online: Over The Counter Lasix – lasix furosemide 40 mg
https://misoprostol.shop/# Misoprostol 200 mg buy online
lasix 100 mg: furosemida – lasix furosemide 40 mg
https://finasteride.men/# generic propecia without insurance
buy misoprostol over the counter: buy cytotec online – cytotec abortion pill
http://finasteride.men/# order generic propecia pills
http://lisinopril.fun/# lisinopril hct
furosemida: Buy Lasix No Prescription – lasix furosemide
generic zithromax medicine zithromax best price how to get zithromax over the counter
http://lisinopril.fun/# where can i get lisinopril
Misoprostol 200 mg buy online: Buy Abortion Pills Online – buy cytotec in usa
propecia without rx: Buy Finasteride 5mg – get propecia pills
https://finasteride.men/# buy generic propecia
cost propecia without insurance: Finasteride buy online – buying cheap propecia online
https://furosemide.pro/# lasix 100mg
https://lisinopril.fun/# lisinopril 40 mg pill
propecia generics buy propecia price rx propecia
buy lisinopril without prescription: lisinopril without rx – buy zestril online
http://misoprostol.shop/# buy cytotec over the counter
rx propecia: Cheapest finasteride online – cost generic propecia without a prescription
where to buy lisinopril 2.5 mg: cheapest lisinopril – lisinopril without prescription
https://furosemide.pro/# lasix generic name
farmacie online sicure avanafil prezzo farmacia online
farmacia online migliore: kamagra oral jelly – acquisto farmaci con ricetta
http://avanafilitalia.online/# farmacie online affidabili
https://avanafilitalia.online/# farmacia online piГ№ conveniente
farmacia online migliore: Avanafil farmaco – farmacia online piГ№ conveniente
http://avanafilitalia.online/# farmacia online più conveniente
http://tadalafilitalia.pro/# comprare farmaci online all’estero
pillole per erezione in farmacia senza ricetta viagra online siti sicuri viagra online in 2 giorni
http://avanafilitalia.online/# acquisto farmaci con ricetta
farmacia online: avanafil – farmacia online senza ricetta
https://farmaciaitalia.store/# farmaci senza ricetta elenco
comprare farmaci online con ricetta: farmacia online miglior prezzo – farmacia online migliore
https://kamagraitalia.shop/# farmacia online migliore
farmacia online piГ№ conveniente cialis prezzo farmaci senza ricetta elenco
miglior sito dove acquistare viagra: sildenafil prezzo – viagra subito
https://farmaciaitalia.store/# acquistare farmaci senza ricetta
viagra online consegna rapida: sildenafil 100mg prezzo – dove acquistare viagra in modo sicuro
farmacia online senza ricetta: Tadalafil prezzo – top farmacia online
http://kamagraitalia.shop/# farmacia online senza ricetta
farmacie on line spedizione gratuita avanafil generico comprare farmaci online con ricetta
https://farmaciaitalia.store/# migliori farmacie online 2023
farmacie online autorizzate elenco: Farmacie a roma che vendono cialis senza ricetta – comprare farmaci online all’estero
https://tadalafilitalia.pro/# comprare farmaci online all’estero
http://mexicanpharm.store/# buying prescription drugs in mexico
mail order pharmacy india: indian pharmacies safe – buy medicines online in india
mexican rx online: medicine in mexico pharmacies – mexican mail order pharmacies
http://indiapharm.life/# top 10 online pharmacy in india
indian pharmacy: top 10 pharmacies in india – world pharmacy india
best india pharmacy: Online medicine home delivery – indian pharmacy
https://mexicanpharm.store/# buying prescription drugs in mexico
canadian pharmacy india: canada online pharmacy – canadian pharmacy
mexican mail order pharmacies reputable mexican pharmacies online mexico pharmacies prescription drugs
http://indiapharm.life/# legitimate online pharmacies india
mexican border pharmacies shipping to usa: medicine in mexico pharmacies – best online pharmacies in mexico
mexican border pharmacies shipping to usa: mexico pharmacy – mexican pharmaceuticals online
https://mexicanpharm.store/# best mexican online pharmacies
https://mexicanpharm.store/# mexican pharmacy
indian pharmacy: п»їlegitimate online pharmacies india – indian pharmacy
http://indiapharm.life/# reputable indian pharmacies
best online pharmacy india: indian pharmacies safe – top 10 pharmacies in india
https://mexicanpharm.store/# best online pharmacies in mexico
top 10 pharmacies in india: buy prescription drugs from india – Online medicine home delivery
onlinecanadianpharmacy: canadian pharmacy ed medications – legit canadian pharmacy online
buy medicines online in india reputable indian pharmacies indian pharmacies safe
http://indiapharm.life/# indian pharmacies safe
india online pharmacy: india pharmacy – buy medicines online in india
https://indiapharm.life/# buy medicines online in india
п»їbest mexican online pharmacies: mexico drug stores pharmacies – mexican border pharmacies shipping to usa
pharmacies in mexico that ship to usa: mexican rx online – pharmacies in mexico that ship to usa
https://mexicanpharm.store/# reputable mexican pharmacies online
https://mexicanpharm.store/# mexican online pharmacies prescription drugs
pet meds without vet prescription canada: pharmacy com canada – online canadian pharmacy review
buy prescription drugs from india: mail order pharmacy india – best india pharmacy
https://indiapharm.life/# cheapest online pharmacy india
mexican mail order pharmacies buying prescription drugs in mexico buying prescription drugs in mexico
mexican mail order pharmacies: buying prescription drugs in mexico – mexican mail order pharmacies
http://indiapharm.life/# top online pharmacy india
best india pharmacy: indian pharmacy – online shopping pharmacy india
https://canadapharm.shop/# best canadian pharmacy to buy from
https://zithromaxpharm.online/# zithromax capsules price
zithromax buy online no prescription: zithromax 1000 mg online – zithromax canadian pharmacy
Their prescription savings club is a godsend http://zithromaxpharm.online/# zithromax for sale us
http://cytotec.directory/# buy cytotec in usa
Their senior citizen discounts are much appreciated http://zithromaxpharm.online/# zithromax for sale 500 mg
nolvadex gynecomastia: where to buy nolvadex – common side effects of tamoxifen
http://zithromaxpharm.online/# generic zithromax azithromycin
tamoxifen endometrium how to lose weight on tamoxifen tamoxifen pill
http://cytotec.directory/# buy cytotec pills
A pharmacy that’s globally recognized and locally loved https://cytotec.directory/# buy cytotec online
http://nolvadex.pro/# tamoxifen bone pain
where can i get clomid without prescription: how to get cheap clomid online – order cheap clomid without a prescription
The best in town, without a doubt http://cytotec.directory/# buy cytotec in usa
https://clomidpharm.shop/# clomid without insurance
zithromax 500 price: zithromax capsules – buy zithromax 500mg online
Drugs information sheet https://cytotec.directory/# Misoprostol 200 mg buy online
cytotec pills buy online cytotec online buy cytotec online fast delivery
http://cytotec.directory/# Cytotec 200mcg price
zithromax canadian pharmacy: where can you buy zithromax – zithromax online pharmacy canada
Their pharmacists are top-notch; highly trained and personable http://zithromaxpharm.online/# order zithromax over the counter
https://clomidpharm.shop/# can you get generic clomid without insurance
http://zithromaxpharm.online/# generic zithromax azithromycin
They have an impressive roster of international certifications https://prednisonepharm.store/# can you buy prednisone over the counter in canada
clomid without insurance: can i buy generic clomid – how to buy clomid price
https://clomidpharm.shop/# clomid pills
Their worldwide outreach programs are commendable https://cytotec.directory/# buy cytotec pills online cheap
buy cytotec over the counter: buy cytotec online – buy cytotec
get generic clomid tablets where buy cheap clomid no prescription buying clomid without dr prescription
http://prednisonepharm.store/# prednisone pharmacy prices
https://reputablepharmacies.online/# onlinecanadianpharmacy com
online ed medications medications for ed medications for ed
canadian pharmacy online http://edpills.bid/# cure ed
mexican pharmacy testosterone
buy prescription drugs online legally: buy prescription drugs from canada – meds online without doctor prescription
https://edwithoutdoctorprescription.store/# real viagra without a doctor prescription
my canadian drug store canadian discount drugs reputable online canadian pharmacy
http://reputablepharmacies.online/# online pharmacy store
cialis without a doctor’s prescription: prescription meds without the prescriptions – non prescription ed pills
canadian mail order drug companies canadian prescription prescription drug discounts
buy cheap prescription drugs online: best non prescription ed pills – prescription drugs online without doctor
international pharmacies: best canadian mail order pharmacy – canadian pharmacy delivery
cheap prescription drugs https://reputablepharmacies.online/# perscription drugs without perscription
recommended online pharmacies
cheap erectile dysfunction pills online treatments for ed drugs for ed
https://edwithoutdoctorprescription.store/# non prescription erection pills
drugs for ed: natural remedies for ed – mens ed pills
canada pharmacy online orders compare pharmacy prices safe online pharmacy
https://reputablepharmacies.online/# canadian pharmacies that are legit
http://edwithoutdoctorprescription.store/# viagra without a doctor prescription
discount mail order pharmacy order from canadian pharmacy internet pharmacy
cialis without doctor prescription: levitra without a doctor prescription – discount prescription drugs
discount prescription drugs: п»їprescription drugs – buy prescription drugs online
real viagra without a doctor prescription usa viagra without a doctor prescription viagra without a doctor prescription
buying prescription drugs canada: canadian drugstore pharmacy – prescription drugs online
http://edwithoutdoctorprescription.store/# prescription drugs canada buy online
generic viagra without a doctor prescription viagra without a doctor prescription walmart ed meds online without doctor prescription
ed pill: best ed treatment – best male enhancement pills
https://edwithoutdoctorprescription.store/# buy prescription drugs online legally
prescription drugs canada buy online ed prescription drugs real cialis without a doctor’s prescription
http://indianpharmacy.shop/# top 10 online pharmacy in india indianpharmacy.shop
canadian pharmacy online reviews Canada Pharmacy prescription drugs canada buy online canadianpharmacy.pro
http://canadianpharmacy.pro/# reputable canadian online pharmacy canadianpharmacy.pro
buying prescription drugs in mexico: mexican pharmacy online – medication from mexico pharmacy mexicanpharmacy.win
http://indianpharmacy.shop/# mail order pharmacy india indianpharmacy.shop
top 10 online pharmacy in india Order medicine from India to USA Online medicine order indianpharmacy.shop
canadian pharmacies compare: Canadian pharmacy online – canadian pharmacy victoza canadianpharmacy.pro
https://indianpharmacy.shop/# india online pharmacy indianpharmacy.shop
canadian pharma companies
purple pharmacy mexico price list mexican pharmacy online mexican pharmaceuticals online mexicanpharmacy.win
https://canadianpharmacy.pro/# canadian pharmacy no rx needed canadianpharmacy.pro
india pharmacy: international medicine delivery from india – india pharmacy indianpharmacy.shop
mexican border pharmacies shipping to usa online mexican pharmacy mexican drugstore online mexicanpharmacy.win
https://mexicanpharmacy.win/# buying prescription drugs in mexico mexicanpharmacy.win
http://canadianpharmacy.pro/# escrow pharmacy canada canadianpharmacy.pro
top 10 pharmacies in india Order medicine from India to USA cheapest online pharmacy india indianpharmacy.shop
https://mexicanpharmacy.win/# mexico drug stores pharmacies mexicanpharmacy.win
https://mexicanpharmacy.win/# mexican border pharmacies shipping to usa mexicanpharmacy.win
indian pharmacy
https://mexicanpharmacy.win/# buying from online mexican pharmacy mexicanpharmacy.win
http://canadianpharmacy.pro/# canadian pharmacy oxycodone canadianpharmacy.pro
canada pharmacies online
canadian pharmacy phone number Canadian pharmacy online safe reliable canadian pharmacy canadianpharmacy.pro
http://mexicanpharmacy.win/# best online pharmacies in mexico mexicanpharmacy.win
top 10 pharmacies in india
https://indianpharmacy.shop/# top 10 pharmacies in india indianpharmacy.shop
http://mexicanpharmacy.win/# mexico drug stores pharmacies mexicanpharmacy.win
online pharmacy india Best Indian pharmacy indian pharmacy paypal indianpharmacy.shop
http://indianpharmacy.shop/# Online medicine home delivery indianpharmacy.shop
online shopping pharmacy india
https://mexicanpharmacy.win/# mexican online pharmacies prescription drugs mexicanpharmacy.win
https://indianpharmacy.shop/# pharmacy website india indianpharmacy.shop
Online medicine home delivery
http://indianpharmacy.shop/# legitimate online pharmacies india indianpharmacy.shop
http://canadianpharmacy.pro/# best canadian pharmacy canadianpharmacy.pro
india online pharmacy
mail order pharmacy india indian pharmacy indianpharmacy com indianpharmacy.shop
http://indianpharmacy.shop/# top 10 pharmacies in india indianpharmacy.shop
https://canadianpharmacy.pro/# reliable canadian pharmacy reviews canadianpharmacy.pro
buy prescription drugs from india
http://canadianpharmacy.pro/# canadian family pharmacy canadianpharmacy.pro
azithromycin canadian pharmacy
the canadian pharmacy Pharmacies in Canada that ship to the US canadian pharmacy online ship to usa canadianpharmacy.pro
https://mexicanpharmacy.win/# mexican pharmacy mexicanpharmacy.win
https://canadianpharmacy.pro/# canadian pharmacy phone number canadianpharmacy.pro
http://canadianpharmacy.pro/# canadian pharmacy service canadianpharmacy.pro
reputable indian pharmacies
trusted canadian pharmacy Canada Pharmacy adderall canadian pharmacy canadianpharmacy.pro
acheter mГ©dicaments Г l’Г©tranger: levitrasansordonnance.pro – Pharmacies en ligne certifiГ©es
https://cialissansordonnance.shop/# pharmacie ouverte 24/24
http://viagrasansordonnance.pro/# Viagra sans ordonnance 24h suisse
п»їpharmacie en ligne
Pharmacies en ligne certifiГ©es Pharmacie en ligne France pharmacie ouverte 24/24
https://viagrasansordonnance.pro/# Viagra générique pas cher livraison rapide
Pharmacie en ligne sans ordonnance pharmacie en ligne sans ordonnance acheter mГ©dicaments Г l’Г©tranger
pharmacie ouverte 24/24: acheterkamagra.pro – Pharmacie en ligne fiable
http://cialissansordonnance.shop/# Pharmacie en ligne France
SildГ©nafil Teva 100 mg acheter: viagrasansordonnance.pro – Meilleur Viagra sans ordonnance 24h
https://pharmadoc.pro/# Pharmacie en ligne sans ordonnance
Pharmacie en ligne sans ordonnance
Viagra pas cher inde Viagra sans ordonnance 24h Viagra prix pharmacie paris
Viagra gГ©nГ©rique sans ordonnance en pharmacie: Viagra Pfizer sans ordonnance – Viagra Pfizer sans ordonnance
http://levitrasansordonnance.pro/# pharmacie ouverte
https://pharmadoc.pro/# Pharmacie en ligne France
acheter medicament a l etranger sans ordonnance cialissansordonnance.shop Pharmacie en ligne France
Viagra gГ©nГ©rique pas cher livraison rapide: viagra sans ordonnance – Viagra sans ordonnance pharmacie France
https://levitrasansordonnance.pro/# Pharmacies en ligne certifiées
Quand une femme prend du Viagra homme Viagra sans ordonnance 24h Viagra prix pharmacie paris
Pharmacie en ligne sans ordonnance: levitra generique – Pharmacies en ligne certifiГ©es
http://viagrasansordonnance.pro/# Viagra sans ordonnance livraison 48h
Acheter mГ©dicaments sans ordonnance sur internet
https://viagrasansordonnance.pro/# Viagra vente libre pays
Pharmacie en ligne France pharmacie en ligne pharmacie ouverte
Sildenafil teva 100 mg sans ordonnance: Acheter du Viagra sans ordonnance – Viagra gГ©nГ©rique pas cher livraison rapide
ivermectin 3: price of ivermectin tablets – ivermectin cost canada
https://prednisonetablets.shop/# where can i buy prednisone without a prescription
cheap amoxicillin 500mg amoxicillin generic amoxicillin order online
54 prednisone: buy prednisone online canada – can i buy prednisone online without prescription
http://prednisonetablets.shop/# prednisone over the counter australia
buy minocycline 50 mg for humans: minocycline manufacturer – minocycline rash
where to buy generic clomid without a prescription: can i buy cheap clomid without prescription – cost of clomid without a prescription
clomid without insurance where to get clomid price where buy cheap clomid without insurance
http://amoxicillin.bid/# order amoxicillin online
http://azithromycin.bid/# zithromax purchase online
where to buy cheap clomid without rx: clomid – how can i get cheap clomid no prescription
stromectol tab ivermectin generic stromectol 6 mg tablet
rexall pharmacy amoxicillin 500mg: amoxicillin 250 mg capsule – how to buy amoxicillin online
where to buy ivermectin: stromectol ivermectin – ivermectin price canada
stromectol otc ivermectin cream 5% ivermectin 18mg
http://azithromycin.bid/# zithromax prescription online
Your article helped me a lot, is there any more related content? Thanks! https://accounts.binance.com/pt-PT/register?ref=S5H7X3LP
ivermectin 400 mg brands: ivermectin 200mg – ivermectin lotion 0.5
https://azithromycin.bid/# average cost of generic zithromax
can you buy amoxicillin over the counter in canada amoxicillin online purchase amoxicillin no prescription
http://clomiphene.icu/# can i buy cheap clomid price
prednisone 3 tablets daily: prednisone 20mg by mail order – 400 mg prednisone
buy zithromax online: zithromax online paypal – zithromax 250 mg australia
http://azithromycin.bid/# zithromax azithromycin
prednisone 5443: can you buy prednisone – prednisone 20 mg tablet
buy amoxil amoxicillin brand name amoxicillin discount
https://amoxicillin.bid/# amoxicillin 500mg price in canada
price for amoxicillin 875 mg: amoxicillin without rx – amoxicillin cost australia
ivermectin 1% stromectol otc stromectol south africa
https://prednisonetablets.shop/# prednisone 20mg online pharmacy
order minocycline 100mg: buy minocycline 100mg for humans – stromectol covid 19
zithromax tablets: zithromax antibiotic – generic zithromax azithromycin
http://amoxicillin.bid/# amoxicillin buy online canada
safe canadian pharmacy: canadian pharmacy oxycodone – certified canadian international pharmacy canadianpharm.store
https://indianpharm.store/# india pharmacy mail order indianpharm.store
legitimate canadian online pharmacies: northwest pharmacy canada – global pharmacy canada canadianpharm.store
india pharmacy international medicine delivery from india online shopping pharmacy india indianpharm.store
canadian online drugstore: Canadian Pharmacy – canadian drugs canadianpharm.store
https://canadianpharm.store/# best canadian pharmacy to buy from canadianpharm.store
purple pharmacy mexico price list: Online Mexican pharmacy – mexican border pharmacies shipping to usa mexicanpharm.shop
canadian pharmacy phone number Best Canadian online pharmacy www canadianonlinepharmacy canadianpharm.store
buying prescription drugs in mexico: Online Pharmacies in Mexico – mexico pharmacy mexicanpharm.shop
https://indianpharm.store/# reputable indian pharmacies indianpharm.store
cheap canadian pharmacy: Canadian International Pharmacy – canadian compounding pharmacy canadianpharm.store
mexican pharmaceuticals online: Online Mexican pharmacy – best online pharmacies in mexico mexicanpharm.shop
indian pharmacy international medicine delivery from india top 10 online pharmacy in india indianpharm.store
http://canadianpharm.store/# canadian pharmacy king canadianpharm.store
http://indianpharm.store/# pharmacy website india indianpharm.store
mexican border pharmacies shipping to usa: Online Mexican pharmacy – mexican rx online mexicanpharm.shop
http://mexicanpharm.shop/# mexican pharmacy mexicanpharm.shop
best rated canadian pharmacy Certified Online Pharmacy Canada cheap canadian pharmacy online canadianpharm.store
mexican pharmacy: mexican rx online – mexico pharmacy mexicanpharm.shop
Online medicine order: indianpharmacy com – reputable indian pharmacies indianpharm.store
india pharmacy: Indian pharmacy to USA – indian pharmacies safe indianpharm.store
http://canadianpharm.store/# reddit canadian pharmacy canadianpharm.store
online pharmacy india buy prescription drugs from india indianpharmacy com indianpharm.store
buying from online mexican pharmacy: mexican rx online – mexican pharmacy mexicanpharm.shop
http://indianpharm.store/# buy prescription drugs from india indianpharm.store
reliable canadian pharmacy: Best Canadian online pharmacy – canadian compounding pharmacy canadianpharm.store
mexico pharmacy Online Mexican pharmacy pharmacies in mexico that ship to usa mexicanpharm.shop
https://mexicanpharm.shop/# reputable mexican pharmacies online mexicanpharm.shop
mexico pharmacies prescription drugs: Online Mexican pharmacy – mexican rx online mexicanpharm.shop
canadian pharmacy service: canadian pharmacy review – canadian pharmacy india canadianpharm.store
canada drugs online reviews: canadapharmacyonline com – canada cloud pharmacy canadianpharm.store
https://canadianpharm.store/# canadian pharmacy review canadianpharm.store
pharmacy com canada Certified Online Pharmacy Canada pet meds without vet prescription canada canadianpharm.store
canadian mail order pharmacy: Canadian Pharmacy – canadian pharmacy online canadianpharm.store
https://indianpharm.store/# top 10 online pharmacy in india indianpharm.store
reputable mexican pharmacies online: Online Mexican pharmacy – п»їbest mexican online pharmacies mexicanpharm.shop
mail order pharmacy india international medicine delivery from india indian pharmacy paypal indianpharm.store
http://canadianpharm.store/# canadian valley pharmacy canadianpharm.store
http://indianpharm.store/# cheapest online pharmacy india indianpharm.store
canadian drug prices: Canada Pharmacy online – canadian neighbor pharmacy canadianpharm.store
п»їbest mexican online pharmacies: Online Pharmacies in Mexico – mexican mail order pharmacies mexicanpharm.shop
pharmacies in mexico that ship to usa Online Pharmacies in Mexico medication from mexico pharmacy mexicanpharm.shop
buying prescription drugs in mexico: buying from online mexican pharmacy – mexican rx online mexicanpharm.shop
Online medicine order: order medicine from india to usa – online pharmacy india indianpharm.store
https://canadianpharm.store/# real canadian pharmacy canadianpharm.store
best canadian online pharmacy Pharmacies in Canada that ship to the US canada cloud pharmacy canadianpharm.store
top online pharmacy india: international medicine delivery from india – india pharmacy mail order indianpharm.store
https://canadianpharm.store/# canadian pharmacy com canadianpharm.store
drugs online: mexican online pharmacy – onlinecanadianpharmacy com
https://canadadrugs.pro/# canadian overnight pharmacy
my canadian pharmacy online: trust pharmacy – online pharmacy no peescription
best canadian online pharmacy viagra cheap canadian drugs canadian discount pharmacy
largest canadian pharmacy: best canadian mail order pharmacy – nabp approved canadian pharmacies
http://canadadrugs.pro/# discount pharmacy coupons
canadian drug pharmacy canadian pharmacies for cialis online pharmacy medications
internet pharmacies: canadian mail order meds – discount pharmaceuticals
cheapest canadian pharmacies: legit canadian pharmacy online – online prescription
http://canadadrugs.pro/# best online pharmacies without prescription
mexican pharmacy drugs: list of online canadian pharmacies – drugs from canada with prescription
top mexican pharmacies international pharmacies online drugstore reviews
certified canadian pharmacy: medication online – internet pharmacy
https://canadadrugs.pro/# canada pharmacy
cheapest canadian pharmacies: cheapest drug prices – canadian pharmacies without prescriptions
most trusted online pharmacy canadian prescription filled in the us canada drug store
https://canadadrugs.pro/# mexican pharmacies online
canadian drug: canadiandrugstore com – buying prescription drugs canada
canadian drug prices: canadian pharmacies top best – canada pharmacy world
https://canadadrugs.pro/# drugstore online
discount drug store online shopping: reputable online canadian pharmacy – canadian pharmacy ship to us
order canadian drugs: canadian world pharmacy – online pharmacy without a prescription
https://canadadrugs.pro/# no prescription drugs canada
best mail order pharmacies: best online pharmacy without prescriptions – best pharmacy
https://canadadrugs.pro/# internet pharmacy no prescription
canada medications online: canadian online pharmacies legitimate by aarp – legal online pharmacies
pharcharmy online no script: canadian pharmaceutical ordering – list of aarp approved pharmacies
https://canadadrugs.pro/# true canadian pharmacy
online pharmacy canada: mexican pharmacy online no prescription – top rated canadian mail order pharmacies
canadian pharmacy ship to us: reputable online canadian pharmacies – canadian pharmacies shipping to usa
https://canadadrugs.pro/# order from canadian pharmacy
pharmacy: online pharmacy no prescriptions – buy medicine canada
https://canadadrugs.pro/# canadian pharmacy no prescrition
reputable online canadian pharmacies: canadian pharmacy order – online pharmacies
ed medications online: erectile dysfunction medicines – best pill for ed
https://edwithoutdoctorprescription.pro/# buy prescription drugs from canada
top ed drugs: male erection pills – ed pills
п»їlegitimate online pharmacies india indianpharmacy com online shopping pharmacy india
legit canadian pharmacy online: canada pharmacy online legit – canadian drug pharmacy
http://edwithoutdoctorprescription.pro/# real cialis without a doctor’s prescription
viagra without a prescription cheap cialis buy prescription drugs online legally
pharmacies in mexico that ship to usa: buying prescription drugs in mexico online – mexico drug stores pharmacies
http://edpill.cheap/# ed drugs compared
top 10 online pharmacy in india: cheapest online pharmacy india – buy prescription drugs from india
canada pharmacy 24h canadian 24 hour pharmacy canadianpharmacymeds com
https://edwithoutdoctorprescription.pro/# prescription drugs online without doctor
http://edwithoutdoctorprescription.pro/# real cialis without a doctor’s prescription
pharmacy website india cheapest online pharmacy india indian pharmacy paypal
https://edwithoutdoctorprescription.pro/# non prescription ed drugs
canadian pharmacy no scripts: canadian pharmacy – reliable canadian online pharmacy
http://edwithoutdoctorprescription.pro/# viagra without doctor prescription amazon
online prescription for ed meds ed pills without doctor prescription prescription drugs canada buy online
mexican rx online: buying prescription drugs in mexico – buying from online mexican pharmacy
http://medicinefromindia.store/# indian pharmacies safe
best online pharmacies in mexico mexican mail order pharmacies medication from mexico pharmacy
buy prescription drugs from canada cheap: generic cialis without a doctor prescription – ed prescription drugs
http://edpill.cheap/# new ed pills
discount prescription drugs buy prescription drugs without doctor best non prescription ed pills
https://edwithoutdoctorprescription.pro/# best non prescription ed pills
mexico pharmacies prescription drugs mexican online pharmacies prescription drugs mexican mail order pharmacies
https://edwithoutdoctorprescription.pro/# buy prescription drugs without doctor
ed pills that work: cheap erectile dysfunction pill – medicine for impotence
https://medicinefromindia.store/# top 10 online pharmacy in india
mexico pharmacies prescription drugs reputable mexican pharmacies online purple pharmacy mexico price list
mexico drug stores pharmacies mexico drug stores pharmacies mexican border pharmacies shipping to usa
http://medicinefromindia.store/# buy prescription drugs from india
cheap canadian pharmacy: canada drugs online – canadian pharmacy
canadian pharmacy no scripts online pharmacy canada canadian pharmacy online
http://edwithoutdoctorprescription.pro/# prescription drugs canada buy online
buying prescription drugs in mexico mexico drug stores pharmacies mexico drug stores pharmacies
https://edwithoutdoctorprescription.pro/# ed meds online without doctor prescription
http://canadianinternationalpharmacy.pro/# canadian pharmacy antibiotics
buying from online mexican pharmacy purple pharmacy mexico price list mexican mail order pharmacies
http://medicinefromindia.store/# reputable indian pharmacies
http://medicinefromindia.store/# best online pharmacy india
online shopping pharmacy india top online pharmacy india reputable indian pharmacies
https://edwithoutdoctorprescription.pro/# non prescription ed pills
real viagra without a doctor prescription usa cheap cialis viagra without a doctor prescription
https://edwithoutdoctorprescription.pro/# prescription drugs canada buy online
indianpharmacy com india pharmacy top 10 pharmacies in india
indian pharmacy paypal: top 10 pharmacies in india – world pharmacy india
http://certifiedpharmacymexico.pro/# buying prescription drugs in mexico
buy cheap prescription drugs online ed pills without doctor prescription viagra without a doctor prescription
https://medicinefromindia.store/# indian pharmacies safe
prescription drugs online without doctor cheap cialis best ed pills non prescription
medication from mexico pharmacy purple pharmacy mexico price list mexican drugstore online
https://mexicanph.shop/# purple pharmacy mexico price list
pharmacies in mexico that ship to usa
medicine in mexico pharmacies mexican pharmacy buying prescription drugs in mexico online
medication from mexico pharmacy buying prescription drugs in mexico mexican pharmacy
mexico drug stores pharmacies mexico pharmacy buying prescription drugs in mexico online
mexico pharmacies prescription drugs mexico drug stores pharmacies purple pharmacy mexico price list
mexican pharmaceuticals online buying from online mexican pharmacy reputable mexican pharmacies online
https://mexicanph.shop/# purple pharmacy mexico price list
buying prescription drugs in mexico
medicine in mexico pharmacies mexico pharmacy mexican pharmaceuticals online
pharmacies in mexico that ship to usa mexican rx online buying from online mexican pharmacy
best online pharmacies in mexico mexican rx online mexico drug stores pharmacies
https://mexicanph.shop/# pharmacies in mexico that ship to usa
best online pharmacies in mexico
mexico drug stores pharmacies purple pharmacy mexico price list medicine in mexico pharmacies
mexican rx online best online pharmacies in mexico mexico pharmacy
mexican online pharmacies prescription drugs mexico drug stores pharmacies mexico pharmacies prescription drugs
pharmacies in mexico that ship to usa mexico pharmacy purple pharmacy mexico price list
best online pharmacies in mexico mexico drug stores pharmacies medication from mexico pharmacy
mexico drug stores pharmacies mexican rx online mexico drug stores pharmacies
mexico pharmacies prescription drugs mexico pharmacies prescription drugs mexican pharmaceuticals online
purple pharmacy mexico price list mexican pharmaceuticals online mexico pharmacies prescription drugs
п»їbest mexican online pharmacies mexican drugstore online mexican pharmacy
http://mexicanph.com/# medication from mexico pharmacy
mexican rx online
mexico pharmacies prescription drugs purple pharmacy mexico price list medicine in mexico pharmacies
mexico pharmacies prescription drugs buying from online mexican pharmacy mexican pharmacy
mexican drugstore online buying prescription drugs in mexico online mexican pharmaceuticals online
pharmacies in mexico that ship to usa buying from online mexican pharmacy mexican pharmacy
buying prescription drugs in mexico mexican rx online buying prescription drugs in mexico online
mexican pharmaceuticals online mexican pharmacy best mexican online pharmacies
medication from mexico pharmacy mexican drugstore online purple pharmacy mexico price list
mexican drugstore online mexican mail order pharmacies mexican drugstore online
purple pharmacy mexico price list pharmacies in mexico that ship to usa buying prescription drugs in mexico
best online pharmacies in mexico mexican border pharmacies shipping to usa mexican pharmacy
mexico drug stores pharmacies medicine in mexico pharmacies pharmacies in mexico that ship to usa
https://mexicanph.shop/# buying prescription drugs in mexico online
medicine in mexico pharmacies
reputable mexican pharmacies online mexico pharmacies prescription drugs mexican drugstore online
mexico drug stores pharmacies reputable mexican pharmacies online buying prescription drugs in mexico
mexico drug stores pharmacies mexico drug stores pharmacies reputable mexican pharmacies online
mexican pharmacy buying from online mexican pharmacy buying prescription drugs in mexico online
mexico drug stores pharmacies mexico drug stores pharmacies mexican drugstore online
reputable mexican pharmacies online mexico pharmacy mexico drug stores pharmacies
buying from online mexican pharmacy pharmacies in mexico that ship to usa medicine in mexico pharmacies
mexican mail order pharmacies mexico pharmacies prescription drugs mexican online pharmacies prescription drugs
medication from mexico pharmacy buying prescription drugs in mexico online mexican online pharmacies prescription drugs
http://mexicanph.shop/# п»їbest mexican online pharmacies
medicine in mexico pharmacies
mexican online pharmacies prescription drugs mexican online pharmacies prescription drugs purple pharmacy mexico price list
mexican border pharmacies shipping to usa mexico pharmacy buying from online mexican pharmacy
buying prescription drugs in mexico buying from online mexican pharmacy mexico pharmacies prescription drugs
mexican rx online mexican border pharmacies shipping to usa mexico pharmacy
buying from online mexican pharmacy mexican drugstore online mexican rx online
best mexican online pharmacies buying from online mexican pharmacy medicine in mexico pharmacies
pharmacies in mexico that ship to usa mexico pharmacy purple pharmacy mexico price list
purple pharmacy mexico price list buying prescription drugs in mexico online mexican drugstore online
mexico pharmacy mexican online pharmacies prescription drugs buying from online mexican pharmacy
mexican pharmacy mexican drugstore online mexican rx online
mexico pharmacies prescription drugs mexico drug stores pharmacies best online pharmacies in mexico
medication from mexico pharmacy medication from mexico pharmacy medicine in mexico pharmacies
https://mexicanph.com/# mexican border pharmacies shipping to usa
mexico drug stores pharmacies
mexico pharmacies prescription drugs mexican pharmaceuticals online reputable mexican pharmacies online
pharmacies in mexico that ship to usa mexican pharmaceuticals online mexico drug stores pharmacies
mexico drug stores pharmacies mexico pharmacy mexican rx online
mexico drug stores pharmacies mexican mail order pharmacies medicine in mexico pharmacies
mexican mail order pharmacies reputable mexican pharmacies online mexico drug stores pharmacies
mexican online pharmacies prescription drugs mexico pharmacies prescription drugs reputable mexican pharmacies online
mexico pharmacies prescription drugs mexican rx online pharmacies in mexico that ship to usa
buying prescription drugs in mexico mexican pharmacy pharmacies in mexico that ship to usa
purple pharmacy mexico price list mexico drug stores pharmacies mexican pharmacy
mexico drug stores pharmacies best online pharmacies in mexico pharmacies in mexico that ship to usa
mexican online pharmacies prescription drugs mexico drug stores pharmacies mexico pharmacies prescription drugs
best online pharmacies in mexico mexican border pharmacies shipping to usa best online pharmacies in mexico
buying prescription drugs in mexico mexican border pharmacies shipping to usa mexican mail order pharmacies
mexican mail order pharmacies mexican online pharmacies prescription drugs best online pharmacies in mexico
medicine in mexico pharmacies mexican pharmacy pharmacies in mexico that ship to usa
mexico drug stores pharmacies mexican rx online pharmacies in mexico that ship to usa
mexican pharmaceuticals online purple pharmacy mexico price list mexican online pharmacies prescription drugs
order prednisone online no prescription: prednisone 5 mg brand name – how to buy prednisone online
amoxicillin online pharmacy: amoxicillin 875 125 mg tab – cost of amoxicillin 875 mg
http://amoxil.cheap/# amoxicillin order online
no prescription online prednisone medicine prednisone 5mg prednisone 40 mg price
http://buyprednisone.store/# prednisone for sale no prescription
ivermectin cost in usa: stromectol tablet 3 mg – п»їwhere to buy stromectol online
http://stromectol.fun/# stromectol order
amoxicillin online without prescription amoxicillin 750 mg price can we buy amoxcillin 500mg on ebay without prescription
order stromectol online: ivermectin 10 ml – buy stromectol online uk
http://furosemide.guru/# buy lasix online
lisinopril 40 mg coupon: url lisinopril hctz prescription – buy lisinopril no prescription
https://lisinopril.top/# lisinopril 20mg tablets
buy amoxicillin 250mg amoxicillin online canada amoxicillin 500mg over the counter
cheap lisinopril no prescription: 10 mg lisinopril cost – lisinopril 20 mg for sale
http://stromectol.fun/# Buy Online Ivermectin/Stromectol Now
30mg prednisone: prednisone uk – prednisone 20 mg tablet
https://furosemide.guru/# lasix 40 mg
buy ivermectin canada: ivermectin uk – stromectol uk
stromectol pill stromectol cost stromectol 3 mg tablet
https://amoxil.cheap/# amoxicillin 500 mg price
canine prednisone 5mg no prescription: prednisone 2.5 mg tab – buy prednisone canadian pharmacy
ivermectin 6mg tablet for lice: ivermectin for humans – ivermectin topical
https://amoxil.cheap/# amoxicillin 500mg pill
buy cheap amoxicillin online amoxicillin 500mg price canada amoxicillin 500mg capsules uk
lasix generic: Buy Lasix – lasix side effects
https://buyprednisone.store/# prednisone for sale
where can i buy amoxicillin over the counter: amoxicillin for sale online – cost of amoxicillin 875 mg
ivermectin 8000 mcg: stromectol drug – ivermectin 3mg tablet
http://stromectol.fun/# generic ivermectin
lasix online Buy Lasix furosemide 100 mg
http://stromectol.fun/# stromectol cream
https://amoxil.cheap/# amoxicillin over counter
amoxicillin 500 mg tablet price: amoxicillin 875 125 mg tab – order amoxicillin uk
https://amoxil.cheap/# buy amoxicillin online no prescription
buy cheap lisinopril 40 mg no prescription: zestoretic 5 mg – order lisinopril online us
can i purchase amoxicillin online how to get amoxicillin canadian pharmacy amoxicillin
prednisone otc price: purchase prednisone canada – prednisone 20 mg tablet price
https://furosemide.guru/# furosemide 100 mg
amoxicillin 500mg for sale uk: buy amoxil – amoxicillin medicine
https://buyprednisone.store/# prednisone daily
zestril 10mg price buy lisinopril no prescription generic zestril
cost of stromectol: how to buy stromectol – ivermectin 500mg
how to buy lisinopril: lisinopril 40 mg discount – 40 mg lisinopril for sale
https://stromectol.fun/# ivermectin cream
https://stromectol.fun/# stromectol generic
http://amoxil.cheap/# order amoxicillin uk
amoxicillin 500 mg brand name: amoxicillin 500 mg tablet – buy amoxil
furosemide 40 mg lasix medication buy lasix online
lisinopril 5mg cost: average cost of lisinopril – lisinopril generic price comparison
https://buyprednisone.store/# prednisone pill
stromectol online: ivermectin 9mg – purchase oral ivermectin
http://amoxil.cheap/# 875 mg amoxicillin cost
lasix generic name Buy Lasix furosemide 100 mg
stromectol tablets uk: price of stromectol – ivermectin 0.08 oral solution
https://stromectol.fun/# buy ivermectin stromectol
lisinopril medication otc: prinivil 25 mg – drug lisinopril 5 mg
https://lisinopril.top/# lisinopril 10 mg no prescription
https://amoxil.cheap/# amoxicillin 500 mg tablet
lasix 20 mg: Buy Lasix No Prescription – lasix dosage
antibiotic amoxicillin amoxicillin without a prescription amoxicillin 500mg capsules uk
https://lisinopril.top/# lisinopril brand
stromectol tablets: ivermectin 0.5 lotion india – ivermectin 0.5
prescription drug prices lisinopril: 40 mg lisinopril – lisinopril 1.25
https://lisinopril.top/# lisinopril 10 mg price in india
ivermectin medicine ivermectin canada ivermectin cream
can i buy amoxicillin online: azithromycin amoxicillin – buy amoxicillin without prescription
http://furosemide.guru/# lasix 100mg
lasix 40 mg: Buy Lasix – buy lasix online
https://buyprednisone.store/# prednisone pill
ivermectin 2mg: ivermectin over the counter – ivermectin over the counter canada
https://amoxil.cheap/# amoxicillin azithromycin
prednisone 10 mg generic prednisone cost 5mg prednisone
https://lisinopril.top/# lisinopril 5
amoxicillin discount coupon: buy amoxicillin 500mg uk – how to buy amoxycillin
http://buyprednisone.store/# purchase prednisone 10mg
lasix: lasix 40 mg – lasix pills
ivermectin 6mg dosage order stromectol buy ivermectin for humans australia
http://buyprednisone.store/# prednisone 30 mg tablet
lasix side effects on kidneys
buy amoxicillin from canada: amoxicillin no prescipion – amoxicillin online canada
https://lisinopril.top/# lisinopril brand name cost
amoxicillin buy no prescription: amoxicillin medicine over the counter – amoxicillin 500 mg capsule
http://buyprednisone.store/# prednisone buy no prescription
prednisone 5 mg cheapest: average cost of generic prednisone – prednisone 10 mg canada
buy amoxicillin from canada amoxacillian without a percription amoxicillin buy canada
http://buyprednisone.store/# prednisone 15 mg daily
amoxicillin tablets in india: how to buy amoxicillin online – amoxacillian without a percription
https://furosemide.guru/# buy lasix online
buy medicines online in india п»їlegitimate online pharmacies india online shopping pharmacy india
amoxicillin 400mg/5ml dosage for child ear infection
https://indianph.com/# indian pharmacy online
indian pharmacy online
india online pharmacy online pharmacy india indian pharmacies safe
india online pharmacy cheapest online pharmacy india top 10 pharmacies in india
http://indianph.xyz/# Online medicine home delivery
india pharmacy
indian pharmacies safe reputable indian pharmacies buy prescription drugs from india
https://indianph.xyz/# buy medicines online in india
india pharmacy mail order
what is amoxicillin
http://indianph.com/# india online pharmacy
http://indianph.xyz/# mail order pharmacy india
cheapest online pharmacy india
indian pharmacy paypal best india pharmacy buy prescription drugs from india
https://indianph.xyz/# pharmacy website india
india pharmacy mail order
buy medicines online in india reputable indian online pharmacy online pharmacy india
https://indianph.xyz/# online pharmacy india
world pharmacy india
http://indianph.com/# buy prescription drugs from india
best online pharmacy india
https://indianph.xyz/# top 10 online pharmacy in india
india pharmacy
reputable indian online pharmacy online shopping pharmacy india india pharmacy mail order
world pharmacy india reputable indian online pharmacy india online pharmacy
https://indianph.com/# buy medicines online in india
reputable indian pharmacies
http://indianph.com/# п»їlegitimate online pharmacies india
buy ciprofloxacin: ciprofloxacin over the counter – cipro online no prescription in the usa
https://nolvadex.guru/# tamoxifen headache
nolvadex 20mg tamoxifen vs raloxifene tamoxifen adverse effects
https://cytotec24.com/# cytotec pills online
Misoprostol 200 mg buy online: buy misoprostol over the counter – cytotec online
https://cytotec24.shop/# order cytotec online
buy doxycycline 100mg doxycycline 150 mg doxycycline generic
buy diflucan yeast infection: how much is over the counter diflucan – diflucan 400mg without prescription
https://nolvadex.guru/# tamoxifen medication
https://nolvadex.guru/# tamoxifen postmenopausal
http://diflucan.pro/# how to buy diflucan
buy cipro cheap п»їcipro generic ciprofloxacin 500mg buy online
ciprofloxacin: cipro ciprofloxacin – ciprofloxacin mail online
https://diflucan.pro/# diflucan 100 mg tab
http://cipro.guru/# ciprofloxacin mail online
ciprofloxacin 500 mg tablet price buy generic ciprofloxacin ciprofloxacin generic
buy cytotec: buy cytotec online – buy cytotec pills online cheap
https://nolvadex.guru/# tamoxifen for gynecomastia reviews
http://cytotec24.shop/# п»їcytotec pills online
http://cytotec24.shop/# buy cytotec online fast delivery
doxy 200 online doxycycline where can i get doxycycline
http://cytotec24.com/# Misoprostol 200 mg buy online
https://cytotec24.shop/# buy cytotec
buy cytotec pills online cheap order cytotec online buy cytotec online
http://cipro.guru/# buy cipro online without prescription
https://cytotec24.shop/# Cytotec 200mcg price
https://cytotec24.com/# cytotec pills buy online
http://cipro.guru/# ciprofloxacin generic price
https://diflucan.pro/# generic diflucan prices
http://nolvadex.guru/# nolvadex pills
http://sweetiefox.online/# Sweetie Fox modeli
Sweetie Fox filmleri: Sweetie Fox filmleri – Sweetie Fox video
https://lanarhoades.fun/# lana rhoades modeli
http://angelawhite.pro/# Angela White video
eva elfie: eva elfie – eva elfie izle
http://lanarhoades.fun/# lana rhoades video
https://abelladanger.online/# abella danger izle
http://evaelfie.pro/# eva elfie video
lana rhoades: lana rhoades izle – lana rhoades filmleri
https://lanarhoades.fun/# lana rhodes
http://angelawhite.pro/# Angela White video
http://abelladanger.online/# abella danger izle
Angela Beyaz modeli: Angela White video – ?????? ????
http://evaelfie.pro/# eva elfie
http://evaelfie.pro/# eva elfie izle
https://angelawhite.pro/# Angela White
Angela White: Abella Danger – Abella Danger
https://lanarhoades.fun/# lana rhoades modeli
https://sweetiefox.online/# Sweetie Fox
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me? https://www.binance.com/zh-TC/register?ref=PORL8W0Z
?????? ????: Angela White izle – Angela White
https://evaelfie.pro/# eva elfie
https://abelladanger.online/# abella danger izle
http://angelawhite.pro/# Angela White video
http://angelawhite.pro/# Angela White filmleri
Angela White video: Abella Danger – abella danger video
https://lanarhoades.fun/# lana rhoades video
https://abelladanger.online/# abella danger izle
Sweetie Fox filmleri: Sweetie Fox modeli – sweety fox
https://abelladanger.online/# Abella Danger
https://evaelfie.pro/# eva elfie filmleri
https://evaelfie.pro/# eva elfie modeli
Sweetie Fox video: Sweetie Fox video – Sweetie Fox modeli
https://abelladanger.online/# abella danger video
http://sweetiefox.online/# sweeti fox
eva elfie modeli: eva elfie video – eva elfie izle
http://angelawhite.pro/# Angela White
https://sweetiefox.online/# swetie fox
https://angelawhite.pro/# Angela White filmleri
http://abelladanger.online/# abella danger izle
https://abelladanger.online/# abella danger filmleri
http://abelladanger.online/# Abella Danger
swetie fox: Sweetie Fox video – Sweetie Fox filmleri
http://evaelfie.pro/# eva elfie video
https://angelawhite.pro/# Angela White izle
?????? ????: Angela White izle – Angela White izle
lana rhodes: lana rhoades – lana rhoades video
https://angelawhite.pro/# Angela White video
http://evaelfie.pro/# eva elfie modeli
http://miamalkova.life/# mia malkova only fans
lana rhoades videos: lana rhoades videos – lana rhoades videos
http://miamalkova.life/# mia malkova hd
mia malkova new video: mia malkova new video – mia malkova movie
https://sweetiefox.pro/# fox sweetie
eva elfie: eva elfie full video – eva elfie hot
eva elfie new video: eva elfie new videos – eva elfie videos
http://evaelfie.site/# eva elfie full videos
online sex chat: http://evaelfie.site/# eva elfie
eva elfie new videos: eva elfie hot – eva elfie hot
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
mia malkova hd: mia malkova only fans – mia malkova hd
https://miamalkova.life/# mia malkova hd
mia malkova new video: mia malkova hd – mia malkova videos
https://miamalkova.life/# mia malkova girl
lana rhoades videos: lana rhoades hot – lana rhoades unleashed
mia malkova photos: mia malkova videos – mia malkova videos
eva elfie full video: eva elfie full videos – eva elfie photo
https://lanarhoades.pro/# lana rhoades boyfriend
connect singles: http://lanarhoades.pro/# lana rhoades videos
eva elfie hot: eva elfie photo – eva elfie new videos
https://miamalkova.life/# mia malkova girl
mia malkova photos: mia malkova movie – mia malkova latest
mia malkova latest: mia malkova videos – mia malkova movie
http://evaelfie.site/# eva elfie new video
dating online free: https://evaelfie.site/# eva elfie full video
sweetie fox cosplay: sweetie fox full video – ph sweetie fox
https://sweetiefox.pro/# sweetie fox full video
mia malkova photos: mia malkova new video – mia malkova hd
sweetie fox new: fox sweetie – fox sweetie
http://sweetiefox.pro/# sweetie fox
sweetie fox full video: sweetie fox full video – ph sweetie fox
online dating simulator: https://miamalkova.life/# mia malkova photos
https://miamalkova.life/# mia malkova videos
mia malkova: mia malkova new video – mia malkova videos
eva elfie hot: eva elfie videos – eva elfie full videos
https://pinupcassino.pro/# aviator oficial pin up
http://pinupcassino.pro/# aviator pin up casino
site de apostas: site de apostas – jogo de aposta
aviator jogar: pin up aviator – aviator jogo
https://aviatoroyunu.pro/# aviator oyunu
aviator jogar: estrela bet aviator – estrela bet aviator
https://aviatorghana.pro/# aviator login
https://aviatorjogar.online/# aviator bet
aviator: aviator betting game – aviator bet malawi
https://jogodeaposta.fun/# aplicativo de aposta
aviator online: como jogar aviator – aviator moçambique
http://aviatormocambique.site/# aviator
http://aviatormocambique.site/# como jogar aviator em mocambique
aviator game bet: aviator login – aviator
como jogar aviator: aviator moçambique – aviator mz
https://pinupcassino.pro/# pin up
aviator bet malawi: aviator game – aviator bet
aviator: aviator sinyal hilesi – pin up aviator
aviator game bet: aviator – aviator betting game
aviator game online: aviator bet – aviator game
http://aviatorghana.pro/# aviator ghana
aviator jogar: aviator betano – jogar aviator Brasil
pin up casino: pin-up casino entrar – pin-up cassino
aviator: aviator bahis – aviator bahis
aviator login: aviator game – aviator game online
aviator hilesi: aviator oyna – aviator hilesi
http://aviatorghana.pro/# aviator bet
jogar aviator: aviator mz – aviator bet
zithromax capsules price: zithromax price canada – zithromax over the counter uk
pin up casino: pin up cassino online – pin up aviator
zithromax capsules australia – https://azithromycin.pro/zithromax-200mg5ml.html can i buy zithromax online
http://jogodeaposta.fun/# melhor jogo de aposta para ganhar dinheiro
aviator pin up: aviator jogo – jogar aviator Brasil
aviator game: play aviator – aviator game online
where can i buy zithromax uk: zithromax online australia – zithromax capsules 250mg
aviator: aviator ghana – aviator sportybet ghana
http://mexicanpharm24.com/# reputable mexican pharmacies online mexicanpharm.shop
india online pharmacy: Top online pharmacy in India – indian pharmacy paypal indianpharm.store
online shopping pharmacy india Online India pharmacy Online medicine home delivery indianpharm.store
india pharmacy: Best Indian pharmacy – pharmacy website india indianpharm.store
mexico pharmacy: mexico drug stores pharmacies – buying prescription drugs in mexico online mexicanpharm.shop
http://mexicanpharm24.shop/# medication from mexico pharmacy mexicanpharm.shop
world pharmacy india Top online pharmacy in India india online pharmacy indianpharm.store
indianpharmacy com: cheapest online pharmacy – indian pharmacy online indianpharm.store
https://canadianpharmlk.com/# best canadian pharmacy online canadianpharm.store
http://canadianpharmlk.com/# vipps canadian pharmacy canadianpharm.store
http://indianpharm24.com/# top online pharmacy india indianpharm.store
medication from mexico pharmacy: mexican pharmacy – medication from mexico pharmacy mexicanpharm.shop
http://canadianpharmlk.shop/# online canadian pharmacy canadianpharm.store
https://canadianpharmlk.shop/# canada drugs online review canadianpharm.store
mexican border pharmacies shipping to usa: Mexico pharmacy online – mexican rx online mexicanpharm.shop
https://canadianpharmlk.com/# canadian pharmacy store canadianpharm.store
https://canadianpharmlk.com/# online canadian pharmacy canadianpharm.store
northern pharmacy canada Canada pharmacy canada pharmacy reviews canadianpharm.store
http://canadianpharmlk.shop/# cheapest pharmacy canada canadianpharm.store
https://canadianpharmlk.com/# thecanadianpharmacy canadianpharm.store
mexico pharmacies prescription drugs: pharmacies in mexico that ship to usa – п»їbest mexican online pharmacies mexicanpharm.shop
http://canadianpharmlk.shop/# legit canadian pharmacy online canadianpharm.store
http://indianpharm24.shop/# reputable indian online pharmacy indianpharm.store
reputable mexican pharmacies online: Mexico pharmacy online – purple pharmacy mexico price list mexicanpharm.shop
https://indianpharm24.shop/# indian pharmacy indianpharm.store
https://canadianpharmlk.shop/# best canadian pharmacy online canadianpharm.store
http://canadianpharmlk.com/# canadian pharmacy ratings canadianpharm.store
https://mexicanpharm24.shop/# buying from online mexican pharmacy mexicanpharm.shop
pharmacy canadian Canada pharmacy online pharmacies in canada that ship to the us canadianpharm.store
indian pharmacies safe: cheapest online pharmacy – world pharmacy india indianpharm.store
https://mexicanpharm24.com/# medication from mexico pharmacy mexicanpharm.shop
http://mexicanpharm24.com/# mexican pharmaceuticals online mexicanpharm.shop
https://canadianpharmlk.shop/# pet meds without vet prescription canada canadianpharm.store
http://indianpharm24.com/# india online pharmacy indianpharm.store
top 10 pharmacies in india: Online India pharmacy – buy prescription drugs from india indianpharm.store
indian pharmacy online: indian pharmacy – mail order pharmacy india indianpharm.store
https://canadianpharmlk.com/# canadian discount pharmacy canadianpharm.store
https://mexicanpharm24.shop/# buying prescription drugs in mexico mexicanpharm.shop
clomid no prescription: can i buy generic clomid now – can i purchase cheap clomid
50 mg prednisone from canada: prednisone otc uk – purchase prednisone canada
https://clomidst.pro/# can i purchase generic clomid without prescription
prednisone 50 mg coupon: buy prednisone without prescription – buy cheap prednisone
get clomid tablets: clomid coupon – how can i get cheap clomid without dr prescription
prednisone 50 mg price order prednisone online canada prednisone 300mg
https://clomidst.pro/# can i buy cheap clomid no prescription
order clomid without dr prescription: clomid without rx – cost generic clomid no prescription
buy prednisone from india: over the counter prednisone cream – prednisone 20mg online
cost of clomid online: where to get generic clomid pill – where can i get cheap clomid without dr prescription
prednisone 40mg: buy prednisone mexico – prednisone 10mg online
https://prednisonest.pro/# buying prednisone on line
amoxicillin tablets in india: how much is amoxicillin – amoxicillin without rx
how can i get generic clomid without insurance: clomid while on trt – get clomid tablets
how to get generic clomid tablets: where can i get clomid now – cost generic clomid without a prescription
prednisone 60 mg: can you take ibuprofen with prednisone – prednisone 25mg from canada
http://clomidst.pro/# where to buy generic clomid no prescription
amoxicillin 500mg price buy amoxicillin 500mg capsules uk generic amoxicillin
where to get cheap clomid price: buying generic clomid tablets – where to buy clomid without insurance
can you buy clomid for sale: order cheap clomid without prescription – clomid cheap
where buy generic clomid prices: can you buy cheap clomid – can i get generic clomid without dr prescription
https://prednisonest.pro/# order prednisone on line
amoxicillin buy no prescription: rexall pharmacy amoxicillin 500mg – generic amoxicillin 500mg
buy prednisone tablets uk: prednisone 20mg price – prednisone buy without prescription
prednisone medication: can you buy prednisone over the counter in canada – buy prednisone online canada
where can i buy cheap clomid: can you buy clomid without a prescription – can i get cheap clomid now
https://amoxilst.pro/# amoxicillin 500
prednisone 40mg: iv prednisone – prednisone drug costs
how to get amoxicillin over the counter amoxicillin online purchase generic amoxicillin
cost of amoxicillin prescription: amoxicillin online canada – medicine amoxicillin 500mg
http://edpills.guru/# what is the cheapest ed medication
mexico prescription drugs online: buy medication online no prescription – buy pain meds online without prescription
online pharmacy non prescription drugs: Best online pharmacy – canadian pharmacy no prescription
http://pharmnoprescription.pro/# discount prescription drugs canada
cheapest prescription pharmacy: canadian online pharmacy – canadian pharmacy coupon
cheap ed treatment: how to get ed pills – online erectile dysfunction medication
https://onlinepharmacy.cheap/# canadian pharmacy coupon code
http://pharmnoprescription.pro/# buying prescription medicine online
ed pills cheap boner pills online ed med online
canadian pharmacy world coupon: mexico pharmacy online – best no prescription pharmacy
canadian online pharmacy no prescription: Best online pharmacy – canadian pharmacy coupon code
https://edpills.guru/# ed meds by mail
cheap ed drugs: cheapest erectile dysfunction pills – discount ed pills
canada drugs coupon code: Cheapest online pharmacy – online pharmacy without prescription
https://onlinepharmacy.cheap/# overseas pharmacy no prescription
canadian pharmacy without prescription: canadian online pharmacy – no prescription required pharmacy
http://pharmnoprescription.pro/# pharmacy online no prescription
best no prescription online pharmacy: no prescription needed – best online pharmacy without prescription
online pharmacy that does not require a prescription: no prescription canadian pharmacy – meds online no prescription
affordable ed medication: buy ed medication online – ed online treatment
online prescription for ed online erectile dysfunction cheap ed meds
https://edpills.guru/# online prescription for ed
https://onlinepharmacy.cheap/# cheapest pharmacy to fill prescriptions with insurance
canadian pharmacy non prescription: prescription from canada – canada mail order prescription
buying prescription drugs in india: pills no prescription – online prescription canada
no prescription: no prescription needed – mexican pharmacies no prescription
buying from online mexican pharmacy: best online pharmacies in mexico – purple pharmacy mexico price list
canadian mail order prescriptions: medications online without prescriptions – best online pharmacies without prescription
http://mexicanpharm.online/# buying prescription drugs in mexico online
top 10 pharmacies in india п»їlegitimate online pharmacies india india pharmacy mail order
pharmacies in mexico that ship to usa: reputable mexican pharmacies online – п»їbest mexican online pharmacies
aspirin for blood pressure
https://canadianpharm.guru/# vipps approved canadian online pharmacy
canada pharmacy online no prescription: buy medications online no prescription – how to get a prescription in canada
https://indianpharm.shop/# top online pharmacy india
Online medicine home delivery: indianpharmacy com – best india pharmacy
aripiprazole tab 2mg
mexican pharmacy: mexican drugstore online – best online pharmacies in mexico
http://mexicanpharm.online/# mexico pharmacy
best online pharmacy india: best online pharmacy india – world pharmacy india
online pharmacy reviews no prescription: overseas online pharmacy-no prescription – non prescription canadian pharmacy
http://indianpharm.shop/# best india pharmacy
canadian pharmacy without a prescription: online medication without prescription – pharmacy no prescription required
online pharmacy india indianpharmacy com cheapest online pharmacy india
http://canadianpharm.guru/# northern pharmacy canada
canadian pharmacies: canada drugstore pharmacy rx – 77 canadian pharmacy
world pharmacy india: top 10 online pharmacy in india – buy medicines online in india
mexico pharmacy: reputable mexican pharmacies online – mexican mail order pharmacies
http://canadianpharm.guru/# canadian online drugs
Online medicine home delivery: reputable indian online pharmacy – indian pharmacy paypal
buying prescription drugs in mexico online: mexican drugstore online – medicine in mexico pharmacies
online pharmacy no prescription: buy medications without a prescription – canada mail order prescription
https://mexicanpharm.online/# mexican pharmaceuticals online
online doctor prescription canada: online canadian pharmacy no prescription – canadian pharmacy online no prescription
http://pharmacynoprescription.pro/# meds online without prescription
buying prescription drugs online from canada buy medication online without prescription buying online prescription drugs
medication from mexico pharmacy: mexican pharmaceuticals online – best mexican online pharmacies
pharmacies in mexico that ship to usa: best online pharmacies in mexico – mexico pharmacy
https://indianpharm.shop/# online pharmacy india
canada pharmacy online legit: canadian pharmacy prices – canadian discount pharmacy
online medication no prescription: best online pharmacy without prescriptions – how to order prescription drugs from canada
how to buy prescriptions from canada safely: online drugs without prescription – canadian prescription prices
http://canadianpharm.guru/# recommended canadian pharmacies
canadian pharmacy: cheap canadian pharmacy online – canadian pharmacy king
buying drugs without prescription: canadian and international prescription service – no prescription pharmacy online
best online pharmacy india: top online pharmacy india – india online pharmacy
https://canadianpharm.guru/# buy canadian drugs
https://canadianpharm.guru/# best canadian online pharmacy
buying drugs from canada canadian online drugstore canada cloud pharmacy
buy pills without prescription: buying prescription medicine online – ordering prescription drugs from canada
mexico drug stores pharmacies: reputable mexican pharmacies online – п»їbest mexican online pharmacies
best online pharmacy no prescription: buying prescription drugs online from canada – non prescription canadian pharmacy
http://indianpharm.shop/# reputable indian online pharmacy
п»їlegitimate online pharmacies india: reputable indian pharmacies – reputable indian pharmacies
canadian pharmacy prices: canadian pharmacy checker – canadian drug pharmacy
no prescription: canadian pharmacy without a prescription – best online prescription
https://canadianpharm.guru/# my canadian pharmacy rx
world pharmacy india: mail order pharmacy india – online shopping pharmacy india
https://canadianpharm.guru/# canadian online drugstore
canadian discount pharmacy: best canadian online pharmacy – canadian neighbor pharmacy
ordering drugs from canada canadian drug pharmacy canadian pharmacy uk delivery
reputable indian pharmacies: best india pharmacy – Online medicine home delivery
buy medications without a prescription: online pharmacy no prescription – canadian prescription prices
https://canadianpharm.guru/# escrow pharmacy canada
my canadian pharmacy: legitimate canadian mail order pharmacy – canada cloud pharmacy
https://indianpharm.shop/# online pharmacy india
purple pharmacy mexico price list: medicine in mexico pharmacies – purple pharmacy mexico price list
buy prescription drugs without a prescription: no prescription medicines – pills no prescription
india pharmacy mail order: cheapest online pharmacy india – Online medicine order
maple leaf pharmacy in canada: canadian pharmacy king – canadian 24 hour pharmacy
http://mexicanpharm.online/# medication from mexico pharmacy
reputable indian online pharmacy: reputable indian online pharmacy – world pharmacy india
https://indianpharm.shop/# Online medicine home delivery
buy medicines online in india indian pharmacy online mail order pharmacy india
reputable mexican pharmacies online: mexico drug stores pharmacies – mexican pharmacy
ordering prescription drugs from canada: meds online no prescription – online prescription canada
online shopping pharmacy india: world pharmacy india – pharmacy website india
https://indianpharm.shop/# indianpharmacy com
canadian pharmacy no prescription required: no prescription medicine – buying prescription drugs online without a prescription
sweet bonanza bahis: sweet bonanza siteleri – sweet bonanza indir
http://slotsiteleri.guru/# deneme bonusu veren slot siteleri
https://gatesofolympus.auction/# gates of olympus s?rlar?
pin up casino: pin up indir – pin-up casino giris
http://pinupgiris.fun/# pin-up online
bonus veren slot siteleri: slot siteleri 2024 – en iyi slot siteleri 2024
https://aviatoroyna.bid/# aviator oyunu 10 tl
sweet bonanza siteleri: sweet bonanza hilesi – sweet bonanza 100 tl
https://gatesofolympus.auction/# gates of olympus demo oyna
http://sweetbonanza.bid/# sweet bonanza free spin demo
https://pinupgiris.fun/# pin up casino
aviator hile: aviator oyunu 10 tl – aviator oyunu 10 tl
pin up aviator: pin-up casino indir – pin up 7/24 giris
http://aviatoroyna.bid/# aviator nasil oynanir
sweet bonanza nas?l oynan?r: sweet bonanza giris – sweet bonanza guncel
http://slotsiteleri.guru/# en iyi slot siteleri 2024
https://sweetbonanza.bid/# sweet bonanza demo turkce
https://gatesofolympus.auction/# gates of olympus demo türkçe oyna
aviator hilesi: aviator sinyal hilesi ucretsiz – aviator
https://gatesofolympus.auction/# gates of olympus demo türkçe oyna
aviator sinyal hilesi: aviator oyna – aviator ucak oyunu
gates of olympus oyna ucretsiz: gates of olympus giris – gates of olympus demo
http://aviatoroyna.bid/# aviator oyna 20 tl
http://sweetbonanza.bid/# sweet bonanza taktik
gates of olympus demo turkce oyna: gates of olympus demo turkce – gates of olympus
https://aviatoroyna.bid/# aviator hile
https://sweetbonanza.bid/# sweet bonanza
en guvenilir slot siteleri: casino slot siteleri – slot casino siteleri
http://pinupgiris.fun/# pin-up giris
gates of olympus demo turkce oyna: gates of olympus nas?l para kazanilir – gates of olympus 1000 demo
https://pinupgiris.fun/# pin up indir
aviator mostbet: aviator oyunu giris – aviator oyunu 10 tl
http://gatesofolympus.auction/# gates of olympus guncel
deneme bonusu veren siteler: en iyi slot siteleri 2024 – en iyi slot siteleri 2024
https://aviatoroyna.bid/# aviator oyunu 10 tl
best online pharmacies in mexico Mexican Pharmacy Online best online pharmacies in mexico
top online pharmacy india: indian pharmacies safe – online pharmacy india
http://canadianpharmacy24.store/# canadian valley pharmacy
buying drugs from canada Large Selection of Medications onlinecanadianpharmacy
mexico pharmacies prescription drugs: Mexican Pharmacy Online – pharmacies in mexico that ship to usa
canadian pharmacy online: pills now even cheaper – reliable canadian online pharmacy
best online pharmacies in mexico mexican pharmacy mexico pharmacy
indian pharmacy paypal: Healthcare and medicines from India – buy medicines online in india
reputable mexican pharmacies online cheapest mexico drugs purple pharmacy mexico price list
canadian pharmacy 1 internet online drugstore: pills now even cheaper – buying drugs from canada
http://canadianpharmacy24.store/# best canadian online pharmacy
india pharmacy mail order: Generic Medicine India to USA – indianpharmacy com
world pharmacy india: Healthcare and medicines from India – cheapest online pharmacy india
online shopping pharmacy india: Cheapest online pharmacy – pharmacy website india
mexican pharmacy buying from online mexican pharmacy buying prescription drugs in mexico online
online pharmacy india: Generic Medicine India to USA – online shopping pharmacy india
pharmacy website india: indian pharmacy delivery – india online pharmacy
india online pharmacy: indian pharmacy online – buy prescription drugs from india
indian pharmacy indian pharmacy reputable indian online pharmacy
canadian discount pharmacy: pills now even cheaper – canadian pharmacy ratings
top online pharmacy india: Healthcare and medicines from India – indian pharmacies safe
https://canadianpharmacy24.store/# the canadian drugstore
online pharmacy india: indian pharmacy delivery – top online pharmacy india
purple pharmacy mexico price list mexico pharmacy reputable mexican pharmacies online
buying prescription drugs in mexico: Online Pharmacies in Mexico – mexican rx online
canadian drugstore online: Prescription Drugs from Canada – my canadian pharmacy
best india pharmacy: Healthcare and medicines from India – india pharmacy
pharmacy website india: Cheapest online pharmacy – best india pharmacy
mexico drug stores pharmacies mexican pharmacy buying from online mexican pharmacy
reputable canadian online pharmacy: Large Selection of Medications – best online canadian pharmacy
indian pharmacy paypal Generic Medicine India to USA indian pharmacies safe
medicine in mexico pharmacies Online Pharmacies in Mexico buying prescription drugs in mexico
mexican pharmacy: reputable mexican pharmacies online – medicine in mexico pharmacies
canada pharmacy world: Licensed Canadian Pharmacy – thecanadianpharmacy
п»їbest mexican online pharmacies: Mexican Pharmacy Online – reputable mexican pharmacies online
reliable canadian pharmacy: canada drugstore pharmacy rx – canada drugs reviews
certified canadian international pharmacy Certified Canadian Pharmacy pharmacy com canada
https://clomidall.com/# how to get generic clomid price
https://clomidall.shop/# how to buy generic clomid without rx
no prescription prednisone canadian pharmacy prednisone prices purchase prednisone 10mg
https://zithromaxall.shop/# buy zithromax online
amoxicillin 500mg capsules uk: where can i buy amoxicillin over the counter – where to get amoxicillin over the counter
buy prednisone nz prednisone online pharmacy over the counter prednisone cheap
https://prednisoneall.shop/# buy prednisone without rx
http://amoxilall.com/# buy amoxicillin canada
http://prednisoneall.com/# prednisone online
generic zithromax online paypal average cost of generic zithromax zithromax cost canada
https://clomidall.shop/# buying generic clomid tablets
http://prednisoneall.shop/# medicine prednisone 10mg
can you buy prednisone online uk where can i buy prednisone prednisone buy online nz
where to buy amoxicillin 500mg: amoxicillin 500 mg capsule – amoxicillin generic
http://zithromaxall.shop/# zithromax 250 mg australia
20 mg prednisone: prednisone canada prescription – prednisone buy cheap
https://clomidall.com/# buy cheap clomid without prescription
buy cheap zithromax online generic zithromax over the counter zithromax
http://zithromaxall.com/# can you buy zithromax over the counter in mexico
https://amoxilall.shop/# amoxicillin no prescipion
can i get clomid without prescription can i purchase generic clomid without dr prescription can i purchase cheap clomid prices
http://prednisoneall.com/# iv prednisone
http://amoxilall.com/# how much is amoxicillin prescription
http://zithromaxall.com/# zithromax tablets for sale
can i get cheap clomid now where can i buy cheap clomid no prescription where to get generic clomid online
get generic clomid now: where can i buy clomid without a prescription – order clomid without a prescription
https://zithromaxall.com/# cost of generic zithromax
prednisone 30 mg tablet: how can i order prednisone – otc prednisone cream
buy prednisone without rx prednisone medicine fast shipping prednisone
http://zithromaxall.com/# generic zithromax online paypal
https://amoxilall.com/# purchase amoxicillin 500 mg
https://prednisoneall.shop/# cheapest prednisone no prescription
amoxicillin 250 mg capsule buy amoxicillin online uk buy amoxicillin 500mg usa
Cheapest Sildenafil online buy viagra online Order Viagra 50 mg online
viagra without prescription: best price on viagra – Viagra online price
https://tadalafiliq.shop/# Generic Tadalafil 20mg price
Kamagra 100mg price: kamagra best price – cheap kamagra
п»їkamagra kamagra best price buy Kamagra
http://tadalafiliq.shop/# Buy Tadalafil 5mg
Kamagra tablets: Kamagra Iq – super kamagra
Cheap Sildenafil 100mg: generic ed pills – Cheap Viagra 100mg
Cheap Viagra 100mg: generic ed pills – sildenafil over the counter
generic sildenafil: best price on viagra – buy Viagra over the counter
abilify ruined my life
https://sildenafiliq.xyz/# generic sildenafil
Sildenafil Citrate Tablets 100mg viagra canada sildenafil over the counter
Kamagra 100mg price: Kamagra 100mg price – buy Kamagra
buy Kamagra: kamagra best price – super kamagra
Cheap generic Viagra online generic ed pills cheapest viagra
https://kamagraiq.shop/# buy kamagra online usa
Sildenafil Citrate Tablets 100mg: sildenafil iq – sildenafil online
http://tadalafiliq.com/# Cialis 20mg price
Cialis 20mg price in USA Generic Tadalafil 20mg price Cialis 20mg price
Kamagra 100mg price: Kamagra Oral Jelly Price – Kamagra 100mg
http://kamagraiq.com/# Kamagra tablets
Viagra tablet online: cheapest viagra – Cheap Viagra 100mg
Kamagra 100mg: Kamagra 100mg – buy kamagra online usa
super kamagra Kamagra gel Kamagra tablets
https://kamagraiq.com/# sildenafil oral jelly 100mg kamagra
Kamagra 100mg price: kamagra best price – Kamagra 100mg price
http://sildenafiliq.xyz/# Cheap generic Viagra
http://sildenafiliq.xyz/# cheap viagra
cialis for sale: cheapest cialis – Generic Cialis without a doctor prescription
Buy Tadalafil 20mg Tadalafil Tablet п»їcialis generic
https://tadalafiliq.shop/# buy cialis pill
Generic Tadalafil 20mg price: cialis best price – cialis generic
https://sildenafiliq.xyz/# viagra canada
Cheap Cialis: cheapest cialis – Cheap Cialis
https://kamagraiq.shop/# cheap kamagra
super kamagra: Kamagra gel – Kamagra 100mg
Buy Cialis online: cheapest cialis – Cheap Cialis
Cheap generic Viagra buy viagra online sildenafil online
https://sildenafiliq.com/# Cheap generic Viagra online
http://kamagraiq.shop/# п»їkamagra
http://kamagraiq.shop/# Kamagra 100mg price
cheap kamagra: Kamagra Oral Jelly – cheap kamagra
the canadian pharmacy CIPA approved pharmacies canadian pharmacy
https://indianpharmgrx.com/# best india pharmacy
mexican rx online: mexican online pharmacies prescription drugs – mexico drug stores pharmacies
online shopping pharmacy india: indian pharmacy – online pharmacy india
mexican rx online Pills from Mexican Pharmacy buying prescription drugs in mexico online
https://indianpharmgrx.com/# mail order pharmacy india
pharmacies in mexico that ship to usa: mexican mail order pharmacies – mexican drugstore online
http://canadianpharmgrx.com/# canada cloud pharmacy
mexican border pharmacies shipping to usa Pills from Mexican Pharmacy buying from online mexican pharmacy
pharmacy website india: buy prescription drugs from india – indian pharmacy
https://mexicanpharmgrx.shop/# buying prescription drugs in mexico
best online pharmacy india Generic Medicine India to USA reputable indian online pharmacy
http://indianpharmgrx.shop/# legitimate online pharmacies india
real canadian pharmacy: Canada pharmacy online – pharmacy in canada
https://mexicanpharmgrx.shop/# mexico drug stores pharmacies
buying prescription drugs in mexico online pharmacy in Mexico medication from mexico pharmacy
indian pharmacy: Generic Medicine India to USA – best online pharmacy india
buy medicines online in india: Generic Medicine India to USA – indian pharmacy
https://indianpharmgrx.shop/# cheapest online pharmacy india
pharmacy canadian superstore International Pharmacy delivery thecanadianpharmacy
https://indianpharmgrx.shop/# buy prescription drugs from india
77 canadian pharmacy Best Canadian online pharmacy pharmacy canadian
mexico drug stores pharmacies: Mexico drugstore – medication from mexico pharmacy
http://mexicanpharmgrx.com/# mexico drug stores pharmacies
india pharmacy mail order: Generic Medicine India to USA – Online medicine home delivery
https://mexicanpharmgrx.com/# buying prescription drugs in mexico online
https://mexicanpharmgrx.com/# medication from mexico pharmacy
indianpharmacy com: indian pharmacy delivery – india pharmacy mail order
canadian world pharmacy: List of Canadian pharmacies – maple leaf pharmacy in canada
mexican border pharmacies shipping to usa Pills from Mexican Pharmacy reputable mexican pharmacies online
http://mexicanpharmgrx.com/# mexican online pharmacies prescription drugs
https://mexicanpharmgrx.shop/# mexico drug stores pharmacies
Online medicine home delivery Healthcare and medicines from India top 10 online pharmacy in india
mexican border pharmacies shipping to usa: best online pharmacies in mexico – purple pharmacy mexico price list
https://mexicanpharmgrx.com/# mexico pharmacies prescription drugs
pharmacies in mexico that ship to usa: Pills from Mexican Pharmacy – mexican drugstore online
buy cipro online without prescription buy generic ciprofloxacin buy generic ciprofloxacin
can i buy diflucan over the counter in australia: diflucan for sale uk – diflucan 250 mg
buy cytotec pills online cheap: buy cytotec – buy cytotec pills online cheap
generic doxycycline doxycycline 150 mg doxycycline 100mg tablets
cipro generic: buy ciprofloxacin – antibiotics cipro
http://doxycyclinest.pro/# doxycycline vibramycin
buy doxycycline online uk: doxycycline 100mg tablets – generic doxycycline
purchase doxycycline online doxycycline hyc doxycycline order online
cipro ciprofloxacin: cipro for sale – buy cipro online
tamoxifen vs raloxifene: tamoxifen lawsuit – tamoxifen dosage
how to get diflucan over the counter diflucan pills online diflucan tablets buy online
tamoxifen alternatives: tamoxifen lawsuit – tamoxifen and bone density
ciprofloxacin mail online: ciprofloxacin over the counter – ciprofloxacin order online
diflucan over the counter: diflucan tablet price – buy generic diflucan
Misoprostol 200 mg buy online Abortion pills online cytotec pills buy online
buy cipro online: cipro for sale – antibiotics cipro
buy cytotec in usa: order cytotec online – purchase cytotec
cipro pharmacy buy generic ciprofloxacin cipro
how much is diflucan over the counter: diflucan 50mg capsules – where to purchase diflucan
buy cytotec pills online cheap: cytotec online – buy cytotec in usa
buy cipro cheap: ciprofloxacin generic price – ciprofloxacin order online
cytotec buy online usa cytotec buy online usa buy cytotec pills online cheap
diflucan uk price: diflucan online australia – generic diflucan prices
doxycycline generic doxy 200 doxycycline hyc 100mg
diflucan canada: diflucan 250 mg – diflucan canada coupon
buy diflucan without prescription: can you buy diflucan in mexico – diflucan over the counter singapore
doxycycline: buy cheap doxycycline – doxycycline without a prescription
https://nolvadex.icu/# does tamoxifen cause joint pain
cytotec pills online: Cytotec 200mcg price – Abortion pills online
doxycycline 150 mg: doxycycline tetracycline – how to order doxycycline
ciprofloxacin generic ciprofloxacin 500mg buy online buy cipro online without prescription
buy doxycycline hyclate 100mg without a rx: doxycycline online – doxylin
diflucan online no prescription: buy diflucan cheap – diflucan cream over the counter
buy cytotec online fast delivery: buy cytotec online – Misoprostol 200 mg buy online
cipro ciprofloxacin buy cipro online canada antibiotics cipro
30mg prednisone: prednisone 15 mg tablet – canada pharmacy prednisone
zithromax buy: can you buy zithromax over the counter in canada – generic zithromax online paypal
can i order generic clomid price: cost cheap clomid no prescription – can i order clomid online
amoxicillin 500mg price in canada buy amoxicillin 500mg amoxicillin discount coupon
prednisone best price: can you buy prednisone over the counter in usa – prednisone buying
https://stromectola.top/# minocycline 100mg tablets
ivermectin lotion price: ivermectin 50mg/ml – buy stromectol uk
https://clomida.pro/# how can i get cheap clomid without insurance
ivermectin new zealand: ivermectin cost in usa – ivermectin 1%
amoxicillin 30 capsules price amoxicillin 750 mg price amoxicillin 500 mg without a prescription
cheap clomid without insurance: cheap clomid without insurance – can i get cheap clomid pills
https://clomida.pro/# where buy clomid for sale
ivermectin 4000 mcg ivermectin australia cost of ivermectin 1% cream
https://amoxicillina.top/# amoxicillin over counter
ordering prednisone: prednisone canada prescription – prednisone pill 10 mg
azithromycin amoxicillin: can we buy amoxcillin 500mg on ebay without prescription – where can you buy amoxicillin over the counter
get clomid online order generic clomid without insurance buy clomid no prescription
where to get clomid without dr prescription: how to buy generic clomid without prescription – where can i buy clomid no prescription
http://azithromycina.pro/# zithromax 250
http://azithromycina.pro/# average cost of generic zithromax
http://medicationnoprescription.pro/# order medication without prescription
buying prescription drugs in canada canadian pharmacy without a prescription no prescription needed online pharmacy
online pharmacy discount code: online pharmacy discount code – rx pharmacy coupons
http://edpill.top/# cheap boner pills
http://onlinepharmacyworld.shop/# legit non prescription pharmacies
purchasing prescription drugs online mexican prescription drugs online online pharmacy not requiring prescription
online prescription canada: best online pharmacy no prescription – buy drugs online without prescription
https://edpill.top/# ed doctor online
https://medicationnoprescription.pro/# meds online no prescription
https://medicationnoprescription.pro/# canadian prescription drugstore reviews
https://edpill.top/# ed medicines
discount ed meds: cheapest ed online – how to get ed meds online
canadian pharmacy without prescription prescription free canadian pharmacy international pharmacy no prescription
https://edpill.top/# ed online prescription
can i buy prescription drugs in canada: buy pain meds online without prescription – online drugs no prescription
http://medicationnoprescription.pro/# online pharmacies no prescription
pills no prescription buy drugs online without prescription online pharmacy canada no prescription
https://medicationnoprescription.pro/# no prescription
https://medicationnoprescription.pro/# meds online no prescription
indian pharmacy no prescription: canada pharmacy no prescription – no prescription pharmacy
erectile dysfunction online: ed pills for sale – cheap ed pills online
cheap ed medicine erectile dysfunction online prescription ed online prescription
https://edpill.top/# get ed meds today
https://edpill.top/# erectile dysfunction meds online
http://casinvietnam.shop/# casino tr?c tuy?n vi?t nam
https://casinvietnam.com/# game c? b?c online uy tin
choi casino tr?c tuy?n tren di?n tho?i casino tr?c tuy?n casino tr?c tuy?n uy tin
http://casinvietnam.shop/# casino online uy tin
casino tr?c tuy?n vi?t nam game c? b?c online uy tin casino online uy tin
dánh bài tr?c tuy?n: casino tr?c tuy?n uy tín – web c? b?c online uy tín
http://casinvietnam.com/# casino tr?c tuy?n vi?t nam
game c? b?c online uy tín: casino tr?c tuy?n uy tín – choi casino tr?c tuy?n trên di?n tho?i
https://casinvietnam.com/# casino tr?c tuy?n uy tin
casino tr?c tuy?n uy tín: dánh bài tr?c tuy?n – dánh bài tr?c tuy?n
game c? b?c online uy tín: dánh bài tr?c tuy?n – web c? b?c online uy tín
web c? b?c online uy tín: choi casino tr?c tuy?n trên di?n tho?i – casino tr?c tuy?n
http://casinvietnam.shop/# danh bai tr?c tuy?n
game c? b?c online uy tín: choi casino tr?c tuy?n trên di?n tho?i – web c? b?c online uy tín
casino tr?c tuy?n: casino tr?c tuy?n – casino tr?c tuy?n
https://casinvietnam.shop/# web c? b?c online uy tin
casino tr?c tuy?n: casino online uy tín – casino tr?c tuy?n vi?t nam
https://casinvietnam.shop/# web c? b?c online uy tin
web c? b?c online uy tín: web c? b?c online uy tín – casino tr?c tuy?n uy tín
web c? b?c online uy tín: choi casino tr?c tuy?n trên di?n tho?i – casino tr?c tuy?n vi?t nam
web c? b?c online uy tín: casino online uy tín – casino online uy tín
http://casinvietnam.shop/# danh bai tr?c tuy?n
casino online uy tín: web c? b?c online uy tín – game c? b?c online uy tín
casino tr?c tuy?n vi?t nam: casino tr?c tuy?n uy tín – choi casino tr?c tuy?n trên di?n tho?i
https://indiaph24.store/# cheapest online pharmacy india
reliable canadian pharmacy: Licensed Canadian Pharmacy – best canadian online pharmacy reviews
https://mexicoph24.life/# medication from mexico pharmacy
http://mexicoph24.life/# mexico pharmacy
http://indiaph24.store/# india pharmacy mail order
https://indiaph24.store/# online shopping pharmacy india
https://canadaph24.pro/# my canadian pharmacy
http://mexicoph24.life/# medication from mexico pharmacy
http://mexicoph24.life/# medicine in mexico pharmacies
https://mexicoph24.life/# best mexican online pharmacies
world pharmacy india: top online pharmacy india – online pharmacy india
https://indiaph24.store/# reputable indian pharmacies
http://canadaph24.pro/# canadian world pharmacy
online pharmacy canada: Large Selection of Medications from Canada – canada drugs online
http://canadaph24.pro/# legitimate canadian online pharmacies
https://canadaph24.pro/# canada drugs reviews
https://indiaph24.store/# indian pharmacy online
https://mexicoph24.life/# mexico pharmacy
indianpharmacy com: indian pharmacy – best online pharmacy india
buying prescription drugs in mexico: mexico pharmacy – mexican drugstore online
http://indiaph24.store/# buy medicines online in india
https://canadaph24.pro/# canada ed drugs
https://canadaph24.pro/# canadian pharmacy 24 com
zyprexa lawsuit settlement
https://canadaph24.pro/# canada drugs
https://mexicoph24.life/# reputable mexican pharmacies online
https://mexicoph24.life/# mexico drug stores pharmacies
http://mexicoph24.life/# purple pharmacy mexico price list
top 10 pharmacies in india: indian pharmacy – india pharmacy mail order
https://mexicoph24.life/# buying from online mexican pharmacy
https://mexicoph24.life/# reputable mexican pharmacies online
https://mexicoph24.life/# pharmacies in mexico that ship to usa
http://canadaph24.pro/# canadian family pharmacy
reputable mexican pharmacies online: Mexican Pharmacy Online – mexico pharmacies prescription drugs
https://canadaph24.pro/# canadian pharmacy antibiotics
http://mexicoph24.life/# reputable mexican pharmacies online
http://indiaph24.store/# top 10 online pharmacy in india
https://indiaph24.store/# buy medicines online in india
www canadianonlinepharmacy: Certified Canadian Pharmacies – canadian pharmacy ratings
https://mexicoph24.life/# mexican mail order pharmacies
https://indiaph24.store/# indian pharmacy
https://mexicoph24.life/# mexican pharmacy
http://canadaph24.pro/# thecanadianpharmacy
п»їlegitimate online pharmacies india: indian pharmacy fast delivery – online pharmacy india
https://indiaph24.store/# Online medicine order
https://mexicoph24.life/# purple pharmacy mexico price list
http://mexicoph24.life/# mexico pharmacy
http://canadaph24.pro/# canada discount pharmacy
indianpharmacy com: pharmacy website india – india pharmacy
https://canadaph24.pro/# canadian pharmacy ratings
http://canadaph24.pro/# best mail order pharmacy canada
http://canadaph24.pro/# canadian pharmacy review
https://indiaph24.store/# indian pharmacy paypal
mexican border pharmacies shipping to usa: mexico pharmacy – mexico pharmacies prescription drugs
https://mexicoph24.life/# mexican drugstore online
http://canadaph24.pro/# canada rx pharmacy world
buying prescription drugs in mexico online: Mexican Pharmacy Online – mexican rx online
https://indiaph24.store/# indian pharmacy online
pet meds without vet prescription canada canadian pharmacies canadian pharmacy victoza
online pharmacy india http://indiaph24.store/# buy prescription drugs from india
indian pharmacy
п»їlegitimate online pharmacies india indian pharmacy fast delivery india pharmacy mail order
buying from online mexican pharmacy: Mexican Pharmacy Online – pharmacies in mexico that ship to usa
https://canadaph24.pro/# legitimate canadian pharmacy online
canadian discount pharmacy: Licensed Canadian Pharmacy – canadian pharmacy online ship to usa
https://indiaph24.store/# reputable indian pharmacies
https://mexicoph24.life/# mexico pharmacies prescription drugs
best online pharmacy india buy medicines from India top 10 online pharmacy in india
https://nolvadex.life/# aromatase inhibitor tamoxifen
tamoxifen headache: femara vs tamoxifen – tamoxifen warning
tamoxifen bone density: nolvadex during cycle – tamoxifen breast cancer
https://nolvadex.life/# tamoxifen and depression
buy cytotec in usa cytotec abortion pill п»їcytotec pills online
https://cytotec.club/# buy cytotec pills
tamoxifen depression liquid tamoxifen should i take tamoxifen
buy lisinopril uk lisinopril 40 mg india lisinopril 90 pills cost
http://nolvadex.life/# tamoxifen and depression
propecia no prescription: cost of generic propecia tablets – buying generic propecia no prescription
Cytotec 200mcg price: Cytotec 200mcg price – cytotec buy online usa
cytotec buy online usa cytotec pills buy online Cytotec 200mcg price
http://nolvadex.life/# tamoxifen rash
cytotec buy online usa buy cytotec online cytotec abortion pill
https://ciprofloxacin.tech/# ciprofloxacin over the counter
https://cytotec.club/# buy cytotec in usa
get generic propecia: buy propecia – cost generic propecia prices
lisinopril 19 mg lisinopril 20 mg canadian pharmacy zestril coupon
Misoprostol 200 mg buy online: buy cytotec pills – Misoprostol 200 mg buy online
ciprofloxacin generic price buy ciprofloxacin ciprofloxacin mail online
https://lisinopril.network/# lisinopril 5 mg brand name in india
tamoxifen for breast cancer prevention tamoxifen mechanism of action tamoxifen and depression
https://ciprofloxacin.tech/# ciprofloxacin over the counter
nolvadex side effects: tamoxifen rash – nolvadex pills
buy misoprostol over the counter purchase cytotec buy cytotec in usa
https://finasteride.store/# cheap propecia online
tamoxifen hot flashes tamoxifen vs clomid what is tamoxifen used for
http://cytotec.club/# buy cytotec in usa
http://cytotec.club/# buy cytotec in usa
get propecia pills: cost of propecia pill – buying propecia without insurance
cytotec online: Misoprostol 200 mg buy online – cytotec pills buy online
tamoxifen cost tamoxifen premenopausal generic tamoxifen
lisinopril tabs 4mg zestril 2.5 prinivil coupon
https://nolvadex.life/# is nolvadex legal
http://lisinopril.network/# lisinopril 15 mg tablets
cipro online no prescription in the usa buy cipro cheap ciprofloxacin
lisinopril tabs: zestril 5mg – lisinopril 50 mg price
ciprofloxacin order online: cipro online no prescription in the usa – ciprofloxacin 500 mg tablet price
buy generic ciprofloxacin cipro 500mg best prices buy cipro cheap
http://finasteride.store/# generic propecia no prescription
ciprofloxacin 500 mg tablet price cipro pharmacy cipro pharmacy
http://ciprofloxacin.tech/# cipro pharmacy
Abortion pills online: cytotec online – buy cytotec over the counter
http://ciprofloxacin.tech/# buy cipro online canada
tamoxifen vs raloxifene: tamoxifen and uterine thickening – does tamoxifen make you tired
buy ciprofloxacin over the counter antibiotics cipro purchase cipro
https://cytotec.club/# buy cytotec in usa
cost of lisinopril 5 mg average cost of lisinopril lisinopril 2.5 mg for sale
https://lisinopril.network/# lisinopril 20 mg tablet cost
https://lisinopril.network/# how to buy lisinopril online
buy generic propecia order generic propecia no prescription cost generic propecia without prescription
buy cytotec online: Abortion pills online – buy cytotec in usa
femara vs tamoxifen: tamoxifen estrogen – tamoxifen buy
lisinopril cost uk zestril pill lisinopril 20mg prices
https://finasteride.store/# get propecia online
cost generic propecia without rx buy generic propecia without insurance cost of propecia without dr prescription
buying generic propecia online: cost of cheap propecia without rx – cost generic propecia for sale
price of lisinopril in india: cost of brand name lisinopril – prinivil
https://finasteride.store/# cost generic propecia prices
buy ciprofloxacin ciprofloxacin 500mg buy online ciprofloxacin order online
alternative to tamoxifen nolvadex steroids where can i buy nolvadex
https://lisinopril.network/# buy lisinopril without a prescription
get cheap propecia pill: buy propecia prices – order cheap propecia pills
cost propecia without insurance: home – buying generic propecia tablets
http://nolvadex.life/# tamoxifen bone density
zestril price lisinopril 10mg prices compare cost for 2 mg lisinopril
purchase cytotec buy cytotec over the counter Abortion pills online
http://cytotec.club/# buy cytotec over the counter
nolvadex half life natural alternatives to tamoxifen does tamoxifen cause menopause
nolvadex price: tamoxifen warning – nolvadex 20mg
buy cytotec over the counter: cytotec abortion pill – order cytotec online
https://ciprofloxacin.tech/# buy ciprofloxacin over the counter
buy cytotec pills buy cytotec in usa buy cytotec over the counter
http://cytotec.club/# buy cytotec pills online cheap
https://cenforce.pro/# buy cenforce
Sildenafil Citrate Tablets 100mg: Buy Viagra online cheap – sildenafil 50 mg price
cialis for sale: Generic Cialis without a doctor prescription – Generic Cialis without a doctor prescription
sildenafil oral jelly 100mg kamagra kamagra oral jelly cheap kamagra
https://cialist.pro/# Buy Tadalafil 20mg
http://cialist.pro/# п»їcialis generic
Cialis 20mg price Generic Cialis without a doctor prescription Cheap Cialis
Kamagra tablets: kamagra – Kamagra 100mg price
https://levitrav.store/# Buy Vardenafil 20mg
buy Kamagra: buy kamagra online – Kamagra 100mg price
Purchase Cenforce Online Cenforce 100mg tablets for sale Buy Cenforce 100mg Online
Levitra generic best price: Levitra generic best price – Levitra 20 mg for sale
buy cenforce Purchase Cenforce Online Purchase Cenforce Online
cheapest cenforce: cheapest cenforce – Cenforce 150 mg online
http://viagras.online/# viagra canada
http://kamagra.win/# super kamagra
http://cialist.pro/# Buy Tadalafil 5mg
Generic Viagra for sale Cheap Viagra 100mg sildenafil over the counter
http://viagras.online/# sildenafil over the counter
kamagra: kamagra oral jelly – sildenafil oral jelly 100mg kamagra
Vardenafil buy online: Vardenafil online prescription – Levitra 10 mg buy online
Buy Tadalafil 5mg buy cialis overseas Cheap Cialis
http://viagras.online/# Cheap generic Viagra
Generic Levitra 20mg Levitra tablet price Buy generic Levitra online
http://viagras.online/# sildenafil 50 mg price
Buy Cenforce 100mg Online: Cenforce 100mg tablets for sale – Buy Cenforce 100mg Online
Cenforce 150 mg online: order cenforce – cenforce.pro
Cheap Sildenafil 100mg Cheapest place to buy Viagra best price for viagra 100mg
Kamagra Oral Jelly: buy kamagra online – Kamagra 100mg price
http://levitrav.store/# Levitra tablet price
buy kamagra online usa kamagra pills Kamagra tablets
https://levitrav.store/# Buy generic Levitra online
Vardenafil online prescription: buy Levitra over the counter – buy Levitra over the counter
Kamagra Oral Jelly sildenafil oral jelly 100mg kamagra Kamagra tablets
buy Viagra over the counter: viagras.online – cheap viagra
kamagra: kamagra – Kamagra Oral Jelly
https://viagras.online/# Viagra online price
https://levitrav.store/# Vardenafil price
Buy Cenforce 100mg Online Purchase Cenforce Online Cenforce 150 mg online
п»їkamagra buy Kamagra cheap kamagra
Buy Tadalafil 10mg: Cialis 20mg price in USA – Generic Cialis price
Cheap generic Viagra: Buy Viagra online – Order Viagra 50 mg online
http://cialist.pro/# Generic Tadalafil 20mg price
buy Levitra over the counter Levitra generic price Levitra tablet price
http://viagras.online/# п»їBuy generic 100mg Viagra online
https://cialist.pro/# cialis for sale
https://pharmmexico.online/# mexican pharmaceuticals online
world pharmacy india: india pharmacy mail order – india pharmacy
canadian pharmacy online ship to usa: canadian family pharmacy – canadian pharmacy
mexican mail order pharmacies medication from mexico pharmacy mexican pharmacy
mexican pharmacy medicine in mexico pharmacies mexico pharmacy
canadian medications: canadian pharmacy in canada – ed meds online canada
http://pharmworld.store/# pharmacy no prescription required
top online pharmacy india: indianpharmacy com – indian pharmacy online
canadian pharmacies comparison: online canadian pharmacy reviews – canadian online pharmacy
pharmacies in mexico that ship to usa: mexican border pharmacies shipping to usa – pharmacies in mexico that ship to usa
canadian pharmacies comparison canadian pharmacy oxycodone canada pharmacy
legal online pharmacy coupon code: online pharmacy – online pharmacy discount code
legal online pharmacy coupon code no prescription needed pharmacy pharmacy discount coupons
https://pharmmexico.online/# mexican drugstore online
cheapest pharmacy prescription drugs: online pharmacy – canadian pharmacy without prescription
best online pharmacy india: Online medicine order – buy prescription drugs from india
online shopping pharmacy india indian pharmacies safe indian pharmacy paypal
reliable canadian pharmacy reviews online pharmacy canada canadapharmacyonline com
canadian pharmacy discount code: pharm world store – best canadian pharmacy no prescription
http://pharmnoprescription.icu/# buy medication online without prescription
purple pharmacy mexico price list: mexico drug stores pharmacies – mexico pharmacies prescription drugs
canadian neighbor pharmacy: canadianpharmacymeds – canadian pharmacy ratings
purple pharmacy mexico price list medication from mexico pharmacy mexico pharmacy
canadapharmacyonline legit: www canadianonlinepharmacy – online canadian drugstore
mexico drug stores pharmacies pharmacies in mexico that ship to usa mexican pharmaceuticals online
order prescription from canada: canadian and international prescription service – prescription drugs online canada
https://pharmcanada.shop/# canadian pharmacy ratings
reputable online pharmacy no prescription: online pharmacy – canadian pharmacy coupon
prescription from canada prescription online canada buy prescription drugs without a prescription
http://pharmnoprescription.icu/# online drugstore no prescription
https://pharmindia.online/# cheapest online pharmacy india
legitimate canadian pharmacy canadian pharmacy near me canada rx pharmacy world
reputable mexican pharmacies online: mexican border pharmacies shipping to usa – buying prescription drugs in mexico online
reputable mexican pharmacies online: mexico drug stores pharmacies – buying prescription drugs in mexico online
purple pharmacy mexico price list: mexican online pharmacies prescription drugs – best online pharmacies in mexico
https://pharmmexico.online/# pharmacies in mexico that ship to usa
canadian drugstore online: canada rx pharmacy – canadian online drugstore
trustworthy canadian pharmacy canadian pharmacy ltd legitimate canadian pharmacy
doxycycline hyclate cheap doxycycline online buy doxycycline online uk
zithromax capsules price: can i buy zithromax over the counter in canada – zithromax capsules price
can i buy zithromax online: generic zithromax medicine – buy zithromax online fast shipping
amoxicillin without prescription: can you buy amoxicillin over the counter canada – purchase amoxicillin online
https://amoxila.pro/# amoxicillin over the counter in canada
doxycycline 100mg price buy doxycycline online 270 tabs buy doxycycline for dogs
where can i buy zithromax capsules: cheap zithromax pills – buy zithromax online
http://amoxila.pro/# generic for amoxicillin
doxycycline 150 mg generic for doxycycline buy doxycycline online uk
how to get zithromax online: zithromax 250 mg pill – zithromax 500 without prescription
purchase amoxicillin online: where can i buy amoxicillin without prec – amoxicillin price without insurance
buy doxycycline monohydrate buy doxycycline hyclate 100mg without a rx doxycycline
buy doxycycline without prescription uk: doxycycline hydrochloride 100mg – doxycycline 100mg price
can you buy zithromax over the counter: zithromax online – generic zithromax medicine
SightCare formula aims to maintain 20/20 vision without the need for any surgical process. This supplement is a perfect solution for people facing issues as they grow older. https://sightcare-web.com/
https://gabapentinneurontin.pro/# discount neurontin
buy amoxicillin online with paypal: order amoxicillin 500mg – cost of amoxicillin 875 mg
buy prednisone online no prescription: prednisone 20mg buy online – can you buy prednisone over the counter in usa
cost of neurontin 100mg: neurontin 2018 – neurontin cream
zithromax 250: zithromax over the counter canada – zithromax 250 mg pill
200 mg doxycycline: where to get doxycycline – doxycycline tetracycline
gabapentin medication: 2000 mg neurontin – neurontin price uk
amoxicillin 500mg price canada: amoxicillin without a prescription – how much is amoxicillin
neurontin uk: cost of brand name neurontin – gabapentin 600 mg
prednisone pack prednisone 20mg tab price medicine prednisone 10mg
neurontin 800 mg tablet 32 neurontin buy neurontin uk
http://zithromaxa.store/# zithromax 500mg price in india
prednisone for sale without a prescription: buy prednisone online no prescription – online order prednisone
purchase amoxicillin online: purchase amoxicillin online – amoxicillin 800 mg price
how much is amoxicillin: amoxicillin 500 mg capsule – where can i buy amoxicillin without prec
where to purchase doxycycline buy generic doxycycline price of doxycycline
neurontin 800 mg neurontin india neurontin pfizer
https://gabapentinneurontin.pro/# neurontin 300 mg tablet
doxycycline without a prescription: odering doxycycline – buy doxycycline 100mg
can you buy zithromax over the counter in australia: zithromax drug – buy zithromax no prescription
buy doxycycline cheap: doxycycline prices – doxycycline 100mg capsules
amoxicillin pills 500 mg where to buy amoxicillin amoxicillin pharmacy price
http://zithromaxa.store/# where can i buy zithromax in canada
PCWer is here to help you with all questions in tech. Whether that
WeJiJ is here to help get you the best gaming setup, gaming PC and guide you through the games you like to play with news, reviews and guides. https://wejij.com/
Easier WWW is a leading technology site that is dedicated to produce great how-to, tips and tricks and cool software review. https://easierwww.com/
Testosil is a natural polyherbal testosterone booster designed to help men increase their testosterone levels safely and effectively. https://testosil-web.com/
neurontin 300 mg 32 neurontin generic neurontin 600 mg
FitSpresso is a natural dietary supplement designed to help with weight loss and improve overall health. It contains ingredients that have been studied clinically, which work together to promote healthy fat burning and enhance your metabolism! https://fitspresso-web.com/
KeraBiotics is a meticulously-crafted natural formula designed to help people dealing with nail fungus. This solution, inspired by a sacred Amazonian barefoot tribe ritual https://kerabiotics-web.com/
Nagano Lean Body Tonic is a groundbreaking powdered supplement crafted to support your weight loss journey effortlessly. https://naganotonic-try.com/
Sugar Defender is a natural supplement that helps control blood sugar levels, lower the risk of diabetes, improve heart health, and boost energy. https://sugardefender-web.com/
– Shoot MASSIVE Loads For An Amazing Finish! https://semenax-try.com/
Tonic Greens is a ready-made greens shake designed to support the entire body and wellness of the mind. It is filled with over 50 individual vitamins https://tonicgreens-try.com/
MenoPhix is a menopause relief supplement featuring a blend of plant extracts to target the root cause of menopause symptoms. https://menophix-web.com/
BalMorex Pro is an exceptional solution for individuals who suffer from chronic joint pain and muscle aches. With its 27-in-1 formula comprised entirely of potent and natural ingredients, it provides unparalleled support for the health of your joints, back, and muscles. https://balmorex-try.com/
https://gabapentinneurontin.pro/# neurontin 100 mg cap
10 mg prednisone: prednisone 25mg from canada – buy prednisone 1 mg mexico
Support the health of your ears with 100% natural ingredients, finally being able to enjoy your favorite songs and movies https://quietumplus-try.com/
Peak BioBoost is a revolutionary dietary supplement that leverages the power of nature to support and improve your digestive system. https://peakbioboost-web.com/
buy doxycycline without prescription: doxycycline medication – buy cheap doxycycline
amoxicillin 500mg capsule: amoxicillin azithromycin – amoxicillin online without prescription
GutOptim is a digestive health supplement designed to support your gut and stomach. It restore balance in gut flora and reduce the symptoms of digestive disorders. https://gutoptim-try.com/
gabapentin 300: neurontin canada – where can i buy neurontin online
zithromax 500mg price in india zithromax 600 mg tablets buy zithromax online australia
Burn Boost Powder™ is a proven weight loss powder drink that helps to lose weight and boosts the overall metabolism in the body. https://burnboost-web.com
NanoDefense Pro utilizes a potent blend of meticulously chosen components aimed at enhancing the wellness of both your nails and skin. https://nanodefense-web.com/
ONLINE EXCLUSIVE OFFER! Only Available for purchase on the official website. Secure Your Package while stocks last https://prodentim-web.com
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
generic amoxicillin 500mg buy amoxicillin 500mg canada buy amoxicillin online mexico
purchase amoxicillin online: amoxicillin 30 capsules price – amoxicillin 500 mg brand name
https://amoxila.pro/# amoxicillin 500mg prescription
amoxicillin without rx how to get amoxicillin amoxicillin cost australia
amoxicillin 500mg capsules: buy amoxicillin canada – buy amoxicillin online cheap
how to get neurontin: neurontin medicine – brand neurontin 100 mg canada
FlowForce Max is an innovative, natural and effective way to address your prostate problems, while addressing your energy, libido, and vitality. https://flowforcemax-web.com/
doxycycline without a prescription odering doxycycline doxycycline hyclate
CLINICALLY PROVEN* To Increase Semen Volume And Intensity https://semenax-try.com/
DuoTrim is an innovative weight loss supplement that utilizes the power of natural plants and nutrients to create CSM bacteria https://duotrim-us.com/
neurontin 50mg tablets: neurontin tablets uk – neurontin mexico
BioFit is a Nutritional Supplement That Uses Probiotics To Help You Lose Weight https://biofit-web.com/
Dentitox Pro is a liquid dietary solution created as a serum to support healthy gums and teeth. Dentitox Pro formula is made in the best natural way with unique, powerful botanical ingredients that can support healthy teeth. https://dentitox-us.com/
Sugar Balance is an ultra-potent blood sugar supplement that you can use to help control glucose levels, melt away fat and improve your overall health. https://sugarbalance-us.com/
GlucoFlush is an advanced formula specially designed for pancreas support that will let you promote healthy weight by effectively maintaining the blood sugar level and cleansing and strengthening your gut. https://glucoflush-us.com/
PureLumin Essence is a meticulously-crafted natural formula designed to help women improve the appearance of age spots. https://pureluminessence-web.com/
http://prednisoned.online/# prednisone tablets india
Alpha Tonic is a powder-based supplement that uses multiple natural herbs and essential vitamins and minerals to help optimize your body’s natural testosterone levels. https://alphatonic-web.com
Vivo Tonic is a remarkable blood sugar support nutritional supplement that offers a wide range of benefits. https://vivotonic-web.com/
odering doxycycline: doxycycline monohydrate – vibramycin 100 mg
prednisone 20 mg prednisone buy without prescription prednisone brand name canada
neurontin 600 mg pill: neurontin 300 mg cap – neurontin 800
Nervogen Pro is an effective dietary supplement designed to help patients with neuropathic pain. When you combine exotic herbs, spices, and other organic substances, your immune system will be strengthened. https://nervogenpro-web.com/
Progenifix is designed to help maximize weight loss results using a mixture of natural, science-backed ingredients. The formula also has secondary benefits, including promoting overall wellness and vitality and assisting your immune system. https://progenifix-web.com/
http://amoxila.pro/# buy amoxicillin 500mg
AquaPeace is an all-natural nutritional formula that uses a proprietary and potent blend of ingredients and nutrients to improve overall ear and hearing health and alleviate the symptoms of tinnitus. https://aquapeace-web.com
neurontin 200 neurontin prescription medication buy neurontin
FoliPrime is a simple serum containing a blend of vitamins designed to boost hair health. FoliPrime has 100 percent natural substances that enhance and supplement the vitamins in the scalp to promote hair growth. https://foliprime-web.com/
prednisone 10 mg tablet: how to get prednisone tablets – prednisone 475
order doxycycline 100mg without prescription: doxycycline tablets – doxycycline 150 mg
Gut Vita™ is a daily supplement that helps consumers to improve the balance in their gut microbiome, which supports the health of their immune system. It supports healthy digestion, even for consumers who have maintained an unhealthy diet for a long time. https://gutvita-us.com/
Fast Lean Pro is a herbal supplement that tricks your brain into imagining that you’re fasting and helps you maintain a healthy weight no matter when or what you eat. It offers a novel approach to reducing fat accumulation and promoting long-term weight management. https://fastleanpro-web.com/
The ProNail Complex is a meticulously-crafted natural formula which combines extremely potent oils and skin-supporting vitamins. https://pronailcomplex-web.com/https://pronailcomplex-web.com/
http://zithromaxa.store/# zithromax prescription online
Erectin is a clinically-proven dietary supplement designed to enhance male https://erectin-web.com/
gabapentin medication: neurontin cost uk – generic gabapentin
doxycycline without a prescription where can i get doxycycline buy doxycycline online 270 tabs
amoxil generic: buying amoxicillin in mexico – amoxicillin 825 mg
PowerBite stands as an innovative dental candy, dedicated to nurturing healthy teeth and gums. Infused with a potent formula, it champions the cause of a robust and radiant smile. Crafted meticulously https://powerbite-web.com/
Protoflow is a prostate health supplement featuring a blend of plant extracts, vitamins, minerals, fruit extracts, and more. https://protoflow-web.com/
https://prednisoned.online/# cost of prednisone 5mg tablets
zithromax capsules australia zithromax tablets for sale zithromax 500 tablet
Cerebrozen is an excellent liquid ear health supplement purported to relieve tinnitus and improve mental sharpness, among other benefits. The Cerebrozen supplement is made from a combination of natural ingredients, and customers say they have seen results in their hearing, focus, and memory after taking one or two droppers of the liquid solution daily for a week. https://cerebrozen-try.com/
200 mg doxycycline: doxycycline generic – doxycycline hyc 100mg
canadian pharmacy amoxicillin: where can i buy amoxicillin over the counter uk – where can i buy amoxicillin without prec
http://doxycyclinea.online/# buy doxycycline without prescription
mail order prednisone: can i buy prednisone online in uk – prednisone 10 mg daily
generic neurontin pill neurontin 202 cost of brand name neurontin
where to buy zithromax in canada: zithromax cost – zithromax without prescription
The human body can continue to live thanks to the correct functioning of certain systems. If even one of these systems does not work properly, it can cause problems in human life. https://calmlean-web.com/
doxycycline without prescription doxycycline 100mg dogs 100mg doxycycline
Zeneara is marketed as an expert-formulated health supplement that can improve hearing and alleviate tinnitus, among other hearing issues. https://zeneara-web.com/
Pineal XT is a revolutionary supplement that promotes proper pineal gland function and energy levels to support healthy body function. https://pinealxt-web.com/
doxycycline 100mg online: vibramycin 100 mg – buy doxycycline monohydrate
VidaCalm is an all-natural blend of herbs and plant extracts that treat tinnitus and help you live a peaceful life. https://vidacalm-web.com/
http://prednisoned.online/# prednisone 50 mg buy
doxycycline 200 mg: buy doxycycline cheap – doxycycline prices
Gorilla Flow prostate is an all-natural dietary supplement for men which aims to decrease inflammation in the prostate to decrease common urinary tract issues such as frequent and night-time urination, leakage, or blocked urine stream. https://gorillaflow-web.com
neurontin tablets 300mg prescription drug neurontin neurontin 1200 mg
3000mg prednisone: how much is prednisone 10 mg – prednisone 10mg prices
zithromax 500 mg: zithromax 500mg over the counter – where can i buy zithromax capsules
HoneyBurn is a revolutionary liquid weight loss formula that stands as the epitome of excellence in the industry. https://honeyburn-web.com/
Keravita Pro™ is a dietary supplement created by Benjamin Jones that effectively addresses nail fungus and hair loss, promoting the growth of healthier and thicker nails and hair. The formula is designed to target the underlying causes of these health issues and provide comprehensive treatment. https://keravitapro-web.com
https://amoxila.pro/# amoxicillin price canada
generic zithromax india order zithromax without prescription zithromax buy
Volca Burn is a weight loss supplement that uses a “red tingle hack” to help you rapidly lose weight without dieting or exercising. https://volcaburn-web.com/
Hydrossential is actually a skincare serum or you can say a skincare supplement created by Emma Smith to help women keep their skin looking beautiful and flawless. https://hydrossential-web.com/
Carbofix is the revolutionary dietary formula that promises to activate weight loss without all the extra hard work. https://carbofix-try.com
Reliver Pro is a dietary supplement formulated with a blend of natural ingredients aimed at supporting liver health
neurontin 100 mg cost: neurontin 4000 mg – neurontin 400
Abdomax is a nutritional supplement using an 8-second Nordic cleanse to eliminate gut issues, support gut health, and optimize pepsinogen levels. https://abdomax-web.com
amoxicillin capsules 250mg: amoxicillin online without prescription – amoxicillin discount
http://amoxila.pro/# can you buy amoxicillin over the counter
how to buy zithromax online buy zithromax canada zithromax capsules price
amoxicillin generic: amoxicillin 50 mg tablets – buy amoxicillin 500mg capsules uk
https://zithromaxa.store/# zithromax 500 without prescription
generic zithromax azithromycin can you buy zithromax over the counter buy generic zithromax no prescription
prednisone 200 mg tablets: can you buy prednisone over the counter uk – prednisone 2.5 mg tab
medicine amoxicillin 500: how to get amoxicillin over the counter – amoxicillin medicine over the counter
amoxicillin 500mg capsule: can you purchase amoxicillin online – amoxicillin discount coupon
http://doxycyclinea.online/# doxycycline generic
buy amoxicillin online no prescription medicine amoxicillin 500mg amoxicillin 500mg over the counter
https://zithromaxa.store/# where can i purchase zithromax online
neurontin 400 neurontin tablets 100mg buy brand neurontin
neurontin generic south africa: neurontin without prescription – neurontin 100mg price
zithromax 500: zithromax antibiotic without prescription – zithromax over the counter canada
zithromax prescription online: buy cheap zithromax online – zithromax 250 price
amoxicillin 500mg capsule buy online: where can i buy amoxicillin without prec – buy amoxicillin
http://zithromaxa.store/# how to get zithromax
zithromax 250 zithromax 500 tablet generic zithromax online paypal
ProstaBiome is a carefully crafted dietary supplement aimed at promoting prostate health. Bid farewell to restless nights and discomfort with ProstaBiome precise strategy for addressing prostate concerns. https://prostabiome-web.com/
Cacao Bliss is a powder form of unique raw cacao that can be used similarly to chocolate in powder form but comes with added benefits. It is designed to provide a rich and satisfying experience while delivering numerous health benefits. https://cacaobliss-web.com/
online prednisone 5mg generic prednisone otc cheapest prednisone no prescription
http://amoxila.pro/# where to get amoxicillin over the counter
buy doxycycline without prescription: price of doxycycline – buy doxycycline cheap
doxycycline hydrochloride 100mg: doxycycline hyc 100mg – doxycycline monohydrate
neurontin india: how much is neurontin – neurontin cost in singapore
prednisone 5mg over the counter prednisone 20 mg tablet prednisone 4mg tab
https://prednisoned.online/# prednisone 20 mg tablet
prednisone 500 mg tablet: buying prednisone on line – prednisone canada prescription
Cneche provides in-depth journalism and insight into the most impactful news and trends shaping the finance industry. https://cneche.com/
can you buy prednisone in canada prednisone 500 mg tablet prednisone over the counter
neurontin cost in canada: neurontin 600 mg capsule – neurontin 800 mg cost
zithromax 500 mg lowest price online: how to buy zithromax online – zithromax online usa no prescription
generic doxycycline doxycycline monohydrate doxycycline
best pharmacy prednisone: prednisone 20mg price – prednisone 10mg for sale
prednisone 10 mg tablets: prednisone 20 mg tablets – prednisone in uk
https://prednisoned.online/# cost of prednisone 40 mg
Lasixiv provides news and analysis for IT executives. We cover big data, IT strategy, cloud computing, security, mobile technology, infrastructure, software and more. https://lasixiv.com
neurontin tablets neurontin pills neurontin 300 mg
order amoxicillin no prescription: can you buy amoxicillin over the counter canada – amoxicillin for sale
http://mexicanpharmacy1st.com/# best online pharmacies in mexico
mexico drug stores pharmacies: purple pharmacy mexico price list – mexico pharmacy
mexican online pharmacies prescription drugs: mexican mail order pharmacies – medicine in mexico pharmacies
п»їbest mexican online pharmacies: buying prescription drugs in mexico – mexico pharmacies prescription drugs
https://mexicanpharmacy1st.com/# best online pharmacies in mexico
п»їbest mexican online pharmacies mexico pharmacies prescription drugs mexican online pharmacies prescription drugs
Wedstraunt has the latest news in the restaurant industry, covering topics like consumer trends, technology, marketing and branding, operations, mergers https://wedstraunt.com
http://mexicanpharmacy1st.com/# reputable mexican pharmacies online
pharmacies in mexico that ship to usa buying from online mexican pharmacy mexican rx online
buying prescription drugs in mexico online: buying from online mexican pharmacy – reputable mexican pharmacies online
https://mexicanpharmacy1st.online/# reputable mexican pharmacies online
mexican border pharmacies shipping to usa: buying prescription drugs in mexico online – mexican mail order pharmacies
Qcmpt provides in-depth journalism and insight into the news and trends impacting the customer experience space. https://qcmpt.com/
mexico drug stores pharmacies pharmacies in mexico that ship to usa п»їbest mexican online pharmacies
pharmacies in mexico that ship to usa: mexican pharmaceuticals online – best mexican online pharmacies
Tvphc provides news and analysis for IT executives. We cover big data, IT strategy, cloud computing, security, mobile technology, infrastructure, software and more. https://tvphc.com
buying prescription drugs in mexico online mexican rx online mexico pharmacy
Ellajon provides news and analysis for construction industry executives. We cover commercial and residential construction, focusing on topics like technology, design, regulation, legal issues and more. https://ellajon.com
https://mexicanpharmacy1st.com/# mexican pharmacy
mexican border pharmacies shipping to usa purple pharmacy mexico price list mexican pharmacy
http://mexicanpharmacy1st.com/# best online pharmacies in mexico
mexican drugstore online: mexico drug stores pharmacies – mexican mail order pharmacies
Grpduk provides news and analysis for human resource executives. We cover topics like recruiting, HR management, employee learning https://grpduk.com
https://mexicanpharmacy1st.online/# mexico pharmacies prescription drugs
medicine in mexico pharmacies: buying prescription drugs in mexico – mexico pharmacy
Susibu provides in-depth journalism and insight into the news and trends impacting the hotel https://susibu.com/
mexico pharmacy reputable mexican pharmacies online buying from online mexican pharmacy
medication from mexico pharmacy mexico pharmacy п»їbest mexican online pharmacies
buying prescription drugs in mexico: purple pharmacy mexico price list – buying prescription drugs in mexico
https://mexicanpharmacy1st.shop/# п»їbest mexican online pharmacies
pharmacies in mexico that ship to usa: best online pharmacies in mexico – medicine in mexico pharmacies
https://mexicanpharmacy1st.online/# mexican drugstore online
https://mexicanpharmacy1st.online/# mexican rx online
Serdar Akar provides in-depth journalism and insight into the news and trends impacting the packaging manufacturing space https://serdarakar.com/
http://mexicanpharmacy1st.com/# buying prescription drugs in mexico
buying prescription drugs in mexico online: mexico pharmacies prescription drugs – purple pharmacy mexico price list
mexico pharmacy: mexico pharmacy – mexican online pharmacies prescription drugs
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://omiyabigan.com/
purple pharmacy mexico price list mexican rx online mexico pharmacies prescription drugs
https://mexicanpharmacy1st.shop/# п»їbest mexican online pharmacies
medicine in mexico pharmacies: buying prescription drugs in mexico – п»їbest mexican online pharmacies
mexican pharmaceuticals online buying prescription drugs in mexico mexican drugstore online
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://smithsis.com
https://mexicanpharmacy1st.com/# medication from mexico pharmacy
medicine in mexico pharmacies: medication from mexico pharmacy – mexico pharmacies prescription drugs
http://mexicanpharmacy1st.com/# mexican pharmacy
purple pharmacy mexico price list mexican border pharmacies shipping to usa mexico pharmacies prescription drugs
Sugar Defender is a revolutionary blood sugar support formula designed to support healthy glucose levels and promote natural weight loss. https://blackboxvending.com/
medicine in mexico pharmacies: mexico drug stores pharmacies – buying from online mexican pharmacy
Sugar Defender is a revolutionary blood sugar support formula designed to support healthy glucose levels and promote natural weight loss. https://mineryuta.com
п»їbest mexican online pharmacies mexico drug stores pharmacies medication from mexico pharmacy
https://mexicanpharmacy1st.shop/# mexico pharmacies prescription drugs
mexican online pharmacies prescription drugs: best online pharmacies in mexico – mexican online pharmacies prescription drugs
purple pharmacy mexico price list: mexican pharmaceuticals online – medication from mexico pharmacy
https://mexicanpharmacy1st.online/# buying prescription drugs in mexico
mexican rx online medication from mexico pharmacy medication from mexico pharmacy
https://mexicanpharmacy1st.shop/# medication from mexico pharmacy
mexico drug stores pharmacies: pharmacies in mexico that ship to usa – best online pharmacies in mexico
mexican rx online: mexico pharmacy – mexican border pharmacies shipping to usa
best online pharmacies in mexico mexico pharmacies prescription drugs mexico pharmacy
Sugar Defender is a revolutionary blood sugar support formula designed to support healthy glucose levels and promote natural weight loss. https://acmesignz.com/
https://mexicanpharmacy1st.shop/# mexican mail order pharmacies
reputable mexican pharmacies online best online pharmacies in mexico reputable mexican pharmacies online
sugar defender: https://novabeaute.com/
sugar defender: https://abmdds.com/
medicine in mexico pharmacies: pharmacies in mexico that ship to usa – buying from online mexican pharmacy
http://mexicanpharmacy1st.com/# mexican pharmacy
pharmacies in mexico that ship to usa: best online pharmacies in mexico – medicine in mexico pharmacies
reputable mexican pharmacies online: medication from mexico pharmacy – mexico drug stores pharmacies
lisinopril 250mg: prinivil coupon – lisinopril 60 mg tablet
sugar defender: https://peyfon.com/
lisinopril 10mg tablet lisinopril 49 mg buy lisinopril canada
sugar defender: https://seahorsesoap.com/
get generic propecia pills cost of generic propecia tablets get generic propecia without rx
zestril 5 mg price: how much is lisinopril 20 mg – lisinopril 420 1g
sugar defender: https://sourceprousa.com/
http://gabapentin.club/# buy neurontin canada
https://lisinopril.club/# lisinopril rx coupon
purchase cytotec: п»їcytotec pills online – Misoprostol 200 mg buy online
https://clomiphene.shop/# order generic clomid for sale
medicine neurontin gabapentin online medicine neurontin 300 mg
lisinopril 10 india lisinopril pills 2.5 mg cost for 2 mg lisinopril
https://cytotec.xyz/# buy cytotec in usa
neurontin tablets uk: neurontin buy from canada – medicine neurontin capsules
neurontin pill neurontin 600mg how much is generic neurontin
neurontin 400mg neurontin cost generic neurontin 500 mg tablet
https://cytotec.xyz/# buy misoprostol over the counter
lisinopril 20 mg purchase: 16 lisinopril – can you order lisinopril online
http://lisinopril.club/# lisinopril 5mg tabs
sugar defender: https://lindadicesare.com/
sugar defender: https://drdenisemichele.com/
sugar defender: https://alchemyfashiongroup.com/
can i order cheap clomid without rx: where can i get cheap clomid pills – where to buy cheap clomid tablets
sugar defender: https://bridgerealtysc.com/
lisinopril tablets uk how to buy lisinopril online lisinopril 12.5 tablet
http://gabapentin.club/# neurontin 800 pill
cytotec online: buy cytotec – cytotec buy online usa
https://lisinopril.club/# order lisinopril 10 mg
neurontin neurontin 300 600 mg neurontin tablets uk
http://clomiphene.shop/# how to buy clomid without rx
buy misoprostol over the counter: cytotec abortion pill – cytotec online
https://gabapentin.club/# gabapentin 300
cost cheap clomid now: where to buy cheap clomid without prescription – where buy clomid no prescription
https://gabapentin.club/# neurontin 4 mg
https://clomiphene.shop/# buying clomid
lisinopril 2.5 lisinopril 20mg buy zestril 10 mg price
buy misoprostol over the counter: buy cytotec over the counter – buy cytotec
cost cheap propecia without a prescription get propecia cost of cheap propecia tablets
how can i get generic clomid online can i get generic clomid without rx how to get generic clomid for sale
http://propeciaf.online/# order cheap propecia without insurance
http://cytotec.xyz/# cytotec buy online usa
propecia without insurance: generic propecia prices – buying propecia without prescription
https://cytotec.xyz/# Cytotec 200mcg price
zestril 10 mg price lisinopril medication cost of lisinopril 2.5 mg
propecia online: cost cheap propecia online – cheap propecia pill
buy cytotec over the counter: buy cytotec online fast delivery – cytotec online
buy propecia without dr prescription cost of cheap propecia no prescription order generic propecia price
http://propeciaf.online/# cost propecia without a prescription
lisinopril 5mg cost: lisinopril 60 mg daily – zestril generic
lisinopril 20mg india zestril 40 lisinopril 125 mg
buying cheap propecia without insurance cost propecia tablets order generic propecia
neurontin prescription cost: neurontin 300 mg price in india – neurontin 400 mg cost
buying generic clomid without dr prescription: can i buy generic clomid without rx – where can i buy generic clomid pill
cost of cheap clomid pills where to get clomid pills how can i get clomid
order neurontin over the counter cost of neurontin 100mg buy generic neurontin
http://gabapentin.club/# neurontin 150mg
online pharmacy non prescription drugs 36 and 6 pharmacy online pharmacy discount code
https://36and6health.shop/# pharmacy no prescription required
https://cheapestcanada.shop/# canadian pharmacy cheap
https://cheapestmexico.shop/# medicine in mexico pharmacies
https://cheapestindia.com/# world pharmacy india
meds online without prescription cheapest and fast no prescription pharmacy
https://cheapestandfast.com/# purchasing prescription drugs online
https://cheapestmexico.com/# mexico pharmacy
mexican mail order pharmacies: medicine in mexico pharmacies – purple pharmacy mexico price list
canada mail order prescription cheapest & fast pharmacy medication online without prescription
https://36and6health.shop/# canadian pharmacy world coupon
http://cheapestcanada.com/# buying from canadian pharmacies
https://cheapestindia.com/# india pharmacy
https://cheapestcanada.shop/# canadian pharmacy victoza
top 10 online pharmacy in india: mail order pharmacy india – reputable indian pharmacies
http://36and6health.com/# foreign pharmacy no prescription
https://cheapestcanada.com/# canadian pharmacy com
best online pharmacy no prescription 36 and 6 pharmacy rx pharmacy coupons
https://36and6health.com/# cheapest pharmacy to get prescriptions filled
http://cheapestindia.com/# top online pharmacy india
canadian online pharmacy no prescription cheapest pharmacy pharmacy coupons
best canadian pharmacy to buy from: canada pharmacy – global pharmacy canada
https://cheapestandfast.com/# mexico online pharmacy prescription drugs
https://cheapestmexico.com/# mexican drugstore online
http://cheapestcanada.com/# canadian pharmacy world
http://cheapestandfast.com/# online doctor prescription canada
best online pharmacy india: indian pharmacies safe – reputable indian online pharmacy
https://cheapestcanada.shop/# canadian pharmacy mall
https://cheapestcanada.com/# canada pharmacy reviews
http://cheapestandfast.com/# how to get a prescription in canada
online shopping pharmacy india india pharmacy online pharmacy india
https://cheapestmexico.com/# mexican pharmacy
https://cheapestandfast.shop/# buy medication online no prescription
http://cheapestmexico.com/# medicine in mexico pharmacies
medicine in mexico pharmacies: mexican pharmaceuticals online – medication from mexico pharmacy
online pharmacy discount code cheapest pharmacy canadian pharmacy no prescription
https://cheapestindia.com/# indian pharmacy
pharmacie en ligne france livraison internationale Achat mГ©dicament en ligne fiable vente de mГ©dicament en ligne
farmacias direct: farmacia online españa envÃo internacional – farmacia online barcelona
apotheke online: europa apotheke – online apotheke versandkostenfrei
online apotheke preisvergleich: ohne rezept apotheke – online apotheke deutschland
https://eumedicamentenligne.com/# vente de mГ©dicament en ligne
vente de mГ©dicament en ligne: pharmacie en ligne avec ordonnance – trouver un mГ©dicament en pharmacie
Farmacia online miglior prezzo: comprare farmaci online con ricetta – Farmacia online piГ№ conveniente
farmacia online senza ricetta: farmacie online autorizzate elenco – farmacia online senza ricetta
günstige online apotheke: online apotheke günstig – apotheke online
farmacias online seguras farmacias online seguras en espaГ±a farmacia barata
https://eumedicamentenligne.com/# pharmacies en ligne certifiГ©es
vente de mГ©dicament en ligne: pharmacie en ligne – Pharmacie en ligne livraison Europe
farmacia online: acquisto farmaci con ricetta – п»їFarmacia online migliore
pharmacie en ligne france: pharmacie en ligne fiable – pharmacie en ligne fiable
online apotheke deutschland: günstige online apotheke – günstigste online apotheke
beste online-apotheke ohne rezept ohne rezept apotheke online apotheke rezept
Pharmacie Internationale en ligne: Pharmacie Internationale en ligne – Pharmacie Internationale en ligne
farmacia online madrid: farmacia online envГo gratis – farmacia online madrid
https://eumedicamentenligne.com/# acheter mГ©dicament en ligne sans ordonnance
farmacia online madrid: farmacia online envÃo gratis – farmacia online 24 horas
farmacie online affidabili acquistare farmaci senza ricetta Farmacie online sicure
farmacia online: Farmacia online piГ№ conveniente – Farmacia online miglior prezzo
online apotheke deutschland: medikamente rezeptfrei – eu apotheke ohne rezept
https://euapothekeohnerezept.com/# ohne rezept apotheke
Farmacie online sicure: farmacia online piГ№ conveniente – acquisto farmaci con ricetta
farmacia online senza ricetta: top farmacia online – farmacie online affidabili
farmacia online barata: farmacia online españa – farmacias direct
top farmacia online п»їFarmacia online migliore farmacia online piГ№ conveniente
gГјnstigste online apotheke: eu apotheke ohne rezept – gГјnstige online apotheke
farmacia online piГ№ conveniente comprare farmaci online con ricetta п»їFarmacia online migliore
pharmacie en ligne fiable: pharmacie en ligne pas cher – trouver un mГ©dicament en pharmacie
Farmacia online piГ№ conveniente: migliori farmacie online 2024 – farmacie online sicure
Pharmacie sans ordonnance: trouver un m̩dicament en pharmacie РPharmacie en ligne livraison Europe
farmacia online più conveniente: farmacia online senza ricetta – farmacie online autorizzate elenco
online apotheke gГјnstig europa apotheke п»їshop apotheke gutschein
pharmacie en ligne france livraison internationale: pharmacie en ligne pas cher – п»їpharmacie en ligne france
internet apotheke: online apotheke versandkostenfrei – apotheke online
http://eufarmacieonline.com/# farmacia online
Farmacia online piГ№ conveniente farmacia online senza ricetta farmacia online senza ricetta
beste online-apotheke ohne rezept: online apotheke – apotheke online
farmacia online barata: farmacia online barcelona – farmacias online seguras en espaГ±a
farmacia online barata y fiable: farmacias online seguras – farmacia online barata y fiable
Pharmacie sans ordonnance: pharmacies en ligne certifiées – pharmacie en ligne france
farmacia online barcelona farmacia en casa online descuento farmacia online espaГ±a envГo internacional
top farmacia online: acquistare farmaci senza ricetta – Farmacie online sicure
apotheke online: europa apotheke – eu apotheke ohne rezept
farmacia online madrid: farmacia barata Рfarmacias online seguras en espa̱a
europa apotheke online apotheke preisvergleich online apotheke
pharmacie en ligne pas cher: pharmacie en ligne livraison europe – pharmacie en ligne pas cher
farmacias online seguras en espaГ±a: farmacia online madrid – farmacia barata
pharmacie en ligne france livraison belgique: pharmacie en ligne france fiable – pharmacie en ligne france pas cher
online apotheke versandkostenfrei: ohne rezept apotheke – internet apotheke
online apotheke gГјnstig: gГјnstige online apotheke – medikament ohne rezept notfall
https://eufarmaciaonline.com/# farmacia online espaГ±a envГo internacional
comprare farmaci online all’estero: farmacia online – farmacie online affidabili
Achat mГ©dicament en ligne fiable pharmacie en ligne pharmacie en ligne
farmacia en casa online descuento: farmacias online seguras en espaГ±a – farmacia online barata
farmacia en casa online descuento: farmacia online envÃo gratis – farmacia online barata
acquisto farmaci con ricetta: acquisto farmaci con ricetta – migliori farmacie online 2024
http://eufarmacieonline.com/# comprare farmaci online con ricetta
farmacia online senza ricetta: п»їFarmacia online migliore – Farmacie online sicure
comprare farmaci online con ricetta top farmacia online Farmacie online sicure
Farmacie on line spedizione gratuita: farmacia online senza ricetta – Farmacie online sicure
Achat mГ©dicament en ligne fiable: cialis prix – pharmacie en ligne france pas cher
https://phenligne.shop/# vente de médicament en ligne
http://cenligne.com/# Pharmacie en ligne livraison Europe
pharmacie en ligne sans ordonnance: pharmacie en ligne sans ordonnance – pharmacie en ligne fiable
Le gГ©nГ©rique de Viagra: Meilleur Viagra sans ordonnance 24h – Viagra homme sans prescription
pharmacie en ligne avec ordonnance: Levitra 20mg prix en pharmacie – trouver un mГ©dicament en pharmacie
Viagra pas cher livraison rapide france Viagra femme ou trouver Viagra 100mg prix
pharmacie en ligne fiable: pharmacie en ligne livraison europe – pharmacie en ligne france fiable
pharmacie en ligne sans ordonnance: levitra generique prix en pharmacie – pharmacies en ligne certifiГ©es
SildГ©nafil 100mg pharmacie en ligne: viagra en ligne – Viagra homme prix en pharmacie sans ordonnance
п»їpharmacie en ligne france pharmacie en ligne pas cher Pharmacie sans ordonnance
Viagra homme prix en pharmacie sans ordonnance: Viagra generique en pharmacie – SildГ©nafil 100 mg sans ordonnance
Viagra gГ©nГ©rique sans ordonnance en pharmacie: Acheter du Viagra sans ordonnance – Viagra pas cher livraison rapide france
trouver un mГ©dicament en pharmacie: Pharmacies en ligne certifiees – pharmacie en ligne fiable
pharmacie en ligne fiable: pharmacie en ligne – pharmacie en ligne avec ordonnance
Prix du Viagra en pharmacie en France viagra en ligne Viagra homme prix en pharmacie sans ordonnance
pharmacies en ligne certifiГ©es: Levitra pharmacie en ligne – pharmacie en ligne pas cher
https://levitraenligne.shop/# pharmacies en ligne certifiées
Achat mГ©dicament en ligne fiable: cialis generique – pharmacie en ligne france fiable
pharmacie en ligne france livraison belgique: Levitra 20mg prix en pharmacie – Achat mГ©dicament en ligne fiable
Hello.
This post was created with XRumer 23 StrongAI.
Good luck 🙂
Viagra pas cher paris: Meilleur Viagra sans ordonnance 24h – Acheter viagra en ligne livraison 24h
Achat mГ©dicament en ligne fiable: kamagra oral jelly – pharmacie en ligne sans ordonnance
pharmacie en ligne fiable: Levitra 20mg prix en pharmacie – Achat mГ©dicament en ligne fiable
Pharmacie sans ordonnance: Levitra 20mg prix en pharmacie – acheter mГ©dicament en ligne sans ordonnance
pharmacie en ligne france livraison belgique: Levitra acheter – pharmacie en ligne avec ordonnance
п»їpharmacie en ligne france: Levitra acheter – trouver un mГ©dicament en pharmacie
acheter mГ©dicament en ligne sans ordonnance: pharmacie en ligne pas cher – trouver un mГ©dicament en pharmacie
pharmacie en ligne fiable: pharmacie en ligne pas cher – pharmacies en ligne certifiГ©es
pharmacie en ligne fiable: pharmacie en ligne – pharmacies en ligne certifiГ©es
Achat mГ©dicament en ligne fiable: cialis prix – pharmacie en ligne france livraison internationale
Viagra Pfizer sans ordonnance: viagra en ligne – Viagra 100mg prix
Viagra homme sans ordonnance belgique: Viagra generique en pharmacie – Viagra 100 mg sans ordonnance
Viagra prix pharmacie paris: viagra sans ordonnance – Viagra sans ordonnance 24h
Hello!
This post was created with XRumer 23 StrongAI.
Good luck 🙂
pharmacie en ligne france livraison belgique: Levitra pharmacie en ligne – pharmacie en ligne sans ordonnance
pharmacie en ligne livraison europe: pharmacie en ligne france fiable – п»їpharmacie en ligne france
pharmacie en ligne fiable: Cialis sans ordonnance 24h – acheter mГ©dicament en ligne sans ordonnance
pharmacie en ligne avec ordonnance: Medicaments en ligne livres en 24h – pharmacie en ligne fiable
SildГ©nafil 100mg pharmacie en ligne: viagra en ligne – Acheter viagra en ligne livraison 24h
Pharmacie en ligne livraison Europe: Levitra pharmacie en ligne – pharmacies en ligne certifiГ©es
pharmacie en ligne avec ordonnance: pharmacie en ligne – pharmacie en ligne
п»їpharmacie en ligne france: kamagra pas cher – pharmacie en ligne france pas cher
vente de mГ©dicament en ligne: levitra generique prix en pharmacie – Pharmacie Internationale en ligne
pharmacie en ligne sans ordonnance: vente de mГ©dicament en ligne – pharmacie en ligne france fiable
trouver un mГ©dicament en pharmacie: Acheter Cialis – vente de mГ©dicament en ligne
Pharmacie en ligne livraison Europe: pharmacie en ligne pas cher – pharmacie en ligne sans ordonnance
vente de mГ©dicament en ligne: cialis prix – acheter mГ©dicament en ligne sans ordonnance
Achat mГ©dicament en ligne fiable: Pharmacies en ligne certifiees – pharmacie en ligne france livraison belgique
pharmacie en ligne fiable: Levitra 20mg prix en pharmacie – Pharmacie Internationale en ligne
п»їpharmacie en ligne france: Acheter Cialis 20 mg pas cher – pharmacie en ligne pas cher
Pharmacie Internationale en ligne: pharmacie en ligne pas cher – Pharmacie en ligne livraison Europe
pharmacie en ligne avec ordonnance: pharmacie en ligne – pharmacie en ligne sans ordonnance
pharmacie en ligne avec ordonnance: cialis generique – pharmacie en ligne france livraison belgique
Pharmacie Internationale en ligne: achat kamagra – pharmacie en ligne pas cher
pharmacie en ligne france livraison internationale: Levitra 20mg prix en pharmacie – pharmacie en ligne france livraison internationale
pharmacie en ligne sans ordonnance: cialis generique – acheter mГ©dicament en ligne sans ordonnance
pharmacie en ligne pas cher: pharmacie en ligne france livraison belgique – vente de mГ©dicament en ligne
pharmacie en ligne france livraison belgique: Acheter Cialis 20 mg pas cher – Pharmacie sans ordonnance
pharmacie en ligne avec ordonnance: kamagra pas cher – Achat mГ©dicament en ligne fiable
Pharmacie sans ordonnance: Medicaments en ligne livres en 24h – pharmacie en ligne fiable
pharmacie en ligne: Pharmacies en ligne certifiees – Pharmacie en ligne livraison Europe
tadalafil liquid review
Viagra gГ©nГ©rique sans ordonnance en pharmacie: viagra sans ordonnance – Viagra sans ordonnance livraison 24h
Achat mГ©dicament en ligne fiable: pharmacie en ligne pas cher – Pharmacie Internationale en ligne
Pharmacie en ligne livraison Europe: Levitra acheter – pharmacie en ligne fiable
Viagra vente libre pays: Viagra femme sans ordonnance 24h – Viagra homme sans ordonnance belgique
vente de mГ©dicament en ligne: kamagra oral jelly – trouver un mГ©dicament en pharmacie
pharmacie en ligne france livraison belgique: pharmacie en ligne sans ordonnance – Pharmacie Internationale en ligne
pharmacie en ligne livraison europe: Pharmacies en ligne certifiees – п»їpharmacie en ligne france
SildГ©nafil 100 mg sans ordonnance: Meilleur Viagra sans ordonnance 24h – Viagra sans ordonnance 24h Amazon
Pharmacie Internationale en ligne: Levitra pharmacie en ligne – pharmacie en ligne france fiable
pharmacie en ligne pas cher: Levitra 20mg prix en pharmacie – pharmacie en ligne
Viagra femme ou trouver: Viagra prix pharmacie paris – Prix du Viagra 100mg en France
acheter mГ©dicament en ligne sans ordonnance: Levitra sans ordonnance 24h – Pharmacie en ligne livraison Europe
Pharmacie Internationale en ligne: levitra generique – pharmacie en ligne
pharmacie en ligne sans ordonnance: Levitra pharmacie en ligne – Pharmacie sans ordonnance
п»їpharmacie en ligne france: kamagra 100mg prix – pharmacie en ligne fiable
pharmacies en ligne certifiГ©es: Cialis sans ordonnance 24h – pharmacie en ligne avec ordonnance
Achat mГ©dicament en ligne fiable: Acheter Cialis 20 mg pas cher – Pharmacie sans ordonnance
https://levitraenligne.shop/# Pharmacie en ligne livraison Europe
http://cenligne.com/# Achat médicament en ligne fiable
Viagra vente libre allemagne: Viagra sans ordonnance 24h – Viagra sans ordonnance livraison 48h
Viagra gГ©nГ©rique pas cher livraison rapide: Viagra homme prix en pharmacie – Sildenafil teva 100 mg sans ordonnance
Acheter Sildenafil 100mg sans ordonnance: viagra sans ordonnance – Sildenafil teva 100 mg sans ordonnance
pharmacie en ligne france livraison internationale: kamagra oral jelly – pharmacie en ligne france livraison belgique
pharmacie en ligne sans ordonnance: Pharmacies en ligne certifiees – pharmacie en ligne france livraison internationale
Pharmacie Internationale en ligne: pharmacie en ligne sans ordonnance – pharmacies en ligne certifiГ©es
Achat mГ©dicament en ligne fiable: Levitra 20mg prix en pharmacie – pharmacie en ligne fiable
pharmacies en ligne certifiГ©es: levitra generique sites surs – Achat mГ©dicament en ligne fiable
pharmacie en ligne sans ordonnance: cialis prix – trouver un mГ©dicament en pharmacie
Achat mГ©dicament en ligne fiable: cialis sans ordonnance – pharmacie en ligne france livraison belgique
pharmacie en ligne livraison europe: levitra generique prix en pharmacie – Pharmacie sans ordonnance
pharmacie en ligne pas cher: acheter kamagra site fiable – acheter mГ©dicament en ligne sans ordonnance
Pharmacie Internationale en ligne: kamagra pas cher – Achat mГ©dicament en ligne fiable
Meilleur Viagra sans ordonnance 24h: Viagra vente libre pays – Viagra sans ordonnance 24h
pharmacie en ligne france fiable: Acheter Cialis 20 mg pas cher – pharmacie en ligne avec ordonnance
pharmacie en ligne france livraison belgique: acheter kamagra site fiable – pharmacie en ligne france livraison belgique
Pharmacie en ligne livraison Europe: Levitra sans ordonnance 24h – pharmacie en ligne france livraison belgique
pharmacie en ligne fiable: pharmacie en ligne – п»їpharmacie en ligne france
https://autolux-azerbaijan.com/# pin-up 141 casino
pin-up 141 casino: Pin Up – Pin-up Giris
https://autolux-azerbaijan.com/# pin-up 141 casino
Pin Up Kazino ?Onlayn: ?Onlayn Kazino – pin-up kazino
Pin Up: Pin Up Azerbaycan ?Onlayn Kazino – pin-up360
https://autolux-azerbaijan.com/# Pin-Up Casino
https://autolux-azerbaijan.com/# Pin Up Azerbaycan
https://autolux-azerbaijan.com/# pin-up360
https://autolux-azerbaijan.com/# Pin Up Kazino ?Onlayn
https://autolux-azerbaijan.com/# pin-up kazino
Pin Up: Pin Up Azerbaycan ?Onlayn Kazino – Pin-Up Casino
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.