LETTER TO EDITOR
Year: 2018 I Volume: 1 I Issue: 3 I Page: 83-86
Comparative Study Of Efficacy and Safety Of Lactic Acid Versus Glycolic Acid Chemical Peels In The Treatment Of Melasma
Sapna Dangi1, Rajkumar Kothiwala2, Ashok Meherda 3
Senior resident, Department of Dermatology, S.M.S Medical College & Hospital, Jaipur
Associate professor, Department of Dermatology, J.L.N. Medical College, Ajmer
Professor, Department of Dermatology, J.L.N. Medical College, Ajmer
Corresponding Author:
Dr. Sapna Dangi
285, A.W.H.O. Colony, Ambabari, Jaipur-302039, Rajasthan
Email: dangi.sapna@gmail.com
How to cite this article:
Dangi S, Kothiwala R, Meherda A. Comparative study of efficacy and safety of Lactic acid versus Glycolic acid chemical peels in the treatment of melasma. JDA Indian Journal of Clinical Dermatology. 2018;1:83-86.
Sir,
Melasma is a common, acquired, symmetric hyperpigmentation commonly involving the cheeks, forehead, upper lip, nose, and chin.1 It predominantly affects women (90%) and is common in individuals with Fitzpatrick skin type IV-VI. Different modalities like keratolytics (tretinoin, resorcin, glycolic, and trichloroacetic acids, etc.) and depigmenting agents (hydroquinone, kojic and azelaic acids) are being used but chemical peeling provides more rapid response than topical therapy.2 Chemical peels create injury at a specific skin depth and causes exfoliation that stimulates new epidermal growth and collagen with more even distribution of melanin.3 Most commonly used peels include phenol, trichloroacetic acid (TCA), alpha hydroxyacids (AHAs), and beta hydroxyacids.
Sixty patients with moderate to severe melasma of epidermal variety only (differentiated by Wood’s lamp examination, according to darkness (D) of pigmentation) were included in the study after getting due ethical clearance from our institute ethics committee. Treatment groups for lactic acid peel and glycolic acid peel were selected randomly and divided into two groups of 30 each. Written informed consent was taken from all the patients included in the study. Cases of dermal melasma were not included in this study because both are superficial to medium depth peels and are not effective for dermal melasma. Patients with a history of herpes, taking oral contraceptive pills or isotretinoin, pregnancy, lactation, history of keloids or hypertrophic scars, concomitant systemic or skin disease and those with unrealistic expectations were excluded from the study.
Melasma Area and Severity Index (MASI) score of the right and left cheeks were calculated for each patient at baseline, at the beginning of each peeling session, and at the end of follow up, along with photography.
The response in each patient was graded as: no response (no change in MASI score at the end of three peels); mild response (less than 25% change); moderate response (25 to <50% decrease in MASI); good response (50 to <75% decrease); very good response (more than 75% decrease). In pre-peel session patients were advised to apply kojic acid 2% or tretinoin 0.025% at night and topical sunscreen daily [SPF-15].
The first group was treated with 35% Glycolic acid after a test peel and second group with 92% Lactic acid. In Glycolic acid group after 3-5 min of application of peeling agent, washing with neutralizer (sodium bicarbonate) was done. In Lactic acid group an erythematous response was awaited within 2 to 3 minutes; if not, then a second layer of application was applied to obtain the desired response and left for 10 minutes after that, it was washed off with water. Peels were performed every 2 weeks for six sessions and participants were instructed to apply sun block cream and emollients. No topical Hypo pigmenting agent was applied. The primary objective of this study was to assess the degree of improvement in pigmentation objectively using MASI at baseline, 2, 4, 6, 8, 10 and 12 weeks. Color photographs were taken of all patients at baseline and 1 month after the last peel.
Paired t-test was used to statistically analyze the change in the mean MASI scoring resulting from treatment in the two groups and to analyze comparative decrease in MASI scoring between the two groups. All the patients in the two groups were examined for any side effects like allergic reactions, hypo or hyperpigmentation, burning, persistent erythema, acneiform eruptions and scarring.
60 patients were included in the study with 54 females and only 6 males, male: female ratio, 1:9. Maximum number of patients was in age group 31-40 year (45%). Mean age of patients in GA group was 32.77±6.88 and in LA group was 30.73±6.03 with p-value of 0.24702 making the two groups statistically comparable. The duration of the disease, in both the groups, in our study ranged from 2 months to 12 years with the mean duration of disease being 3.04±1.927 years in group 1 (Glycolic acid group) and 2.79±2.69years in group 2 (Lactic acid group). The difference between the mean duration of disease in the two groups was statistically not significant (p=0.6687), thus both the groups were comparable in terms of duration of disease. Most common pattern observed was Centro facial (58.3%) followed by malar 35% [Figure 1]. Only 15% patients gave family history of melasma. Pregnancy had no significant association with melasma and only 11(18.3%) patients gave a history of occurrence of melasma during pregnancy.
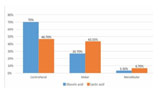 |
Figure 1: Clinical pattern of melasma in both Glycolic acid and Lactic acid group. |
Objective response to treatment was measured by a decrease in MASI scoring after each peel session. Up to 2 week (1 peel) there was no significant response in both the groups (p>.05). After 12 weeks reduction in MASI was 54% (from 22.29 to 10.12) in GA group (Figure 2a, 2b and 3a, 3b) and 68% (from 22.15 to 6.91) in LA group (Figure 4a, 4band 5a, 5b) which was highly significant (p<.001). The MASI scores at baseline, 2 4, 6 8, 10 12 weeks were as shown in [Figure 6].
Thus lactic acid 92% showed better efficacy compared to Glycolic acid 35%. When we assessed the adverse effects, the frequency of serious adverse effects was very low in both the groups [Figure7]. Common adverse effects were mild burning (36.67% of patients in LA group and 50% in Glycolic acid group) only at the time of application of peel but resolved after ice cooling, calamine application and use of sunscreens. Erythema (6.67% in LA and 20% in GA) which resolved after applying 1% hydrocortisone cream for 3-4 days and hyperpigmentation was seen in 3.33% in GA but none of the patient in LA group.
Recurrence at 3 months follow up was seen in 25 patients in GA group in form of increase in MASI score which was significant (p<.05). No relapse was seen in LA group.
Melasma is a symmetric progressive hyperpigmentation of the facial skin that occurs in all races but observed more frequently in darker skin phenotypes. There are three clinical patterns –
 |
Figure 2a, 2b: Melasma in 35 year old female before and after treatment with GA peel. |
 |
Figure 3a, 3b: Melasma in 30 year old male before and after treatment with GA peel. |
centrofacial, malar, and mandibular – depending upon the area of localization.1 By Wood’s light examination, melasma can be classified into epidermal, dermal or mixed type. Different modalities as depigmenting agents, laser, and chemical peeling have been used alone and in combination for the treatment of melasma.4 Chemical peels are often used as an adjunct to medical treatment because they produce complementary rapid therapeutic effects and improves skin appearance and texture.5 Peels allow topical agents to penetrate more efficiently into the skin and may improve post inflammatory hyperpigmentation.6
Chemical peels create controlled chemical burn of the skin and produces partial thickness wound that heals by secondary intention. The end results are thinning of stratum corneum, epidermolysis, dispersion of basal layer melanin, regulation of epidermal thickness and laying down of new collagen and ground substance in dermis.7 Depending upon the depth of peeling achieved, the chemical peeling agents are classified into very superficial, superficial, medium and deep peels.8 Chemical peels useful in treating melasma are trichloroacetic acid, Jessner’s
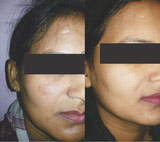 |
Figure 4a, 4b: Melasma in 28 year old female before and after treatment with LA peel. |
 |
Figure 5a, 5b: Melasma in 25 year old female before and after treatment with LA peel. |
solution, alpha-hydroxy acid preparations, and salicylic acid, alone or in various combinations. Alpha-hydroxy-acids (AHAs) have been the most commonly used agents for superficial peelings. Both the agents used in this study, LA 92% and GA 35%, are superficial peels.
Glycolic acid (GA) is obtained from sugarcane and is the simplest and most-used alpha-hydroxy acid peel.9 GA is a popular peel agent because it has the smallest molecular weight amongst all the alpha-hydroxy acids and penetrates skin easily.6 Fabbrocini, in 2009, classified glycolic peels as: very superficial (30%–50% GA, applied for 1–2 minutes); superficial (50%–70% GA, applied for 2–5 minutes); and medium depth (70% GA, applied for 3–15 minutes).10 GA peels have anti-inflammatory, keratolytic, and antioxidant effects. GA targets the corneosome by enhancing breakdown and decreasing cohesiveness, causing desquamation.11 GA peels need to be properly neutralized to stop acidification of the skin. In a study by Sarkar et al, modified Kligman’s formula (2% hydroquinone, 0.025% tretinoin, and 1% mometasone), was compared with GA peels (30% GA for the first three sittings; 40% GA for the next three sittings), combined with the modified Kligman’s formula and GA peel group showed more rapid and greater improvement (P < 0.001).2
Alpha hydroxy acids have been used as effective peeling agents in a variety of conditions including melasma, but the clinical
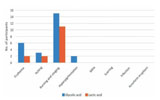 |
Figure 6: Comparison between change in Mean MASI score of Glycolic acid and Lactic acid with treatment duration. |
experience is limited to glycolic acid only,12 which is expensive and may not be available in every center.13 Lactic acid, also an alphahydroxy acid having activities similar to GA, it is a non-costly and readily available agent but has not been used extensively as a peeling agent in the treatment of melasma. Further, because of its large molecular size, there is less penetration with an additional advantage of being more hydrating and less irritating.14 The first study in melasma was done by Sharquie et al.15 and found it to be a safe and effective peeling agent for melasma in dark skin. In their study of 20 patients, 92% pure lactic acid was applied for a maximum of six sessions, and a significant fall in MASI (56%) was observed in all the 12 patients who completed the study. Further, LA was compared with Jessner’s solution in melasma, and and it was as effective as Jessner’s solution.16
 |
Figure 6: Comparison of adverse effects of peel in both the groups. |
However, the clinical experience of LA peeling in melasma is very limited and to the best of our knowledge, there is no study available in the literature comparing the efficacy and safety of Lactic acid peeling with Glycolic acid peeling in melasma. This prompted us to undertake a clinical trial comparing the efficacy and safety of Lactic acid peeling with Glycolic acid peeling in the treatment of melasma.
Limitation of our study was short follow up period of 3 months only so we were not able to detect late recurrences that may also occur in LA peel. Both the Glycolic acid 35% and Lactic acid 92% are effective peeling agents in epidermal melasma. Both significantly reduces MASI scores (p<.001). At the end of treatment LA peel showed better efficacy with rapid rate of clinical improvement. Side effects were seen with both peeling agents but less commonly with LA. Side effects were mild and not significant. More studies need to be conducted with different concentrations of GA and Lactic acid on larger samples and in other pigmentary disorders.
References:
1. Lapeere H, Boone B, Schepper SD, Verhaeghe E, Ongenae K, Geel NV, et al. Hypomelanosis and hypermelanosis. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick’s Dermatology in General Medicine. 7 th ed. New York: McGraw-Hill; 2008. P. 622-40
2. Sarkar R, Kaur C, Bhalla M, Kanwar AJ. The combination of glycolic acid peels with a topical regimen in the treatment of melasma in Dark-skinned patients: a comparative study. Dermatol Surg 2002; 28(9): 828-32.
3. Ghersetich I, Teofoll P, Gantcheva M, Ribuffo M, Puddu P. Chemical peeling: How, when, why? J Eur Acad Dermatol Venererol 1997; 8: 1–11.
4. Ortonne JP, Passeron T. Melanin pigmentary disorders: Treatment update. Dermatol Clin 2005; 23(5): 209–26.
5. Atzori L, Brundu MA, Orru A, Biggio P. Glycolic acid peeling in the treatment of acne. J Eur Acad Dermatol Venereol 1999; 12(2):119–22.
6. Landau M. Chemical peels. Clin Dermatol. 2008; 26(2): 200–8.
7. Savant SS, Mehta N. Superficial and medium depth chemical peeling. In: Savant SS, Atal SR, Gore D, editors. Textbook and atlas of dermatosurgery and cosmetology. 2nd ed. Philadelphia: WB Saunders Company; 2005. p. 177-95.
8. Rubin MG. What are skin peels? In: Winters SR, James M, Caputa GR, editors. Manual of chemical peels – superficial and medium depth. Philadelphia: Lippincott Williams & Wilkins; 1995. p. 17-25.
9. Khunger N, editor. Step by Step Chemical Peels. 2nd edn. Delhi, India: Jaypee Brothers; 2014. p. 61.
10. Fabbrocini G, De Padova MP, Tosti A. Chemical peels: what’s new and what isn’t new but still works well. Facial Plast Surg 2009; 25(5): 329–36.
11. Fartasch M, Teal J, Menon GK. Mode of action of glycolic acid on human stratum corneum: ultrastructural and functional evaluation of the epidermal barrier. Arch Dermatol Res 1997; 289 (7): 404–09.
12. Verallo-Rowell VM, Verallo V, Graupe K, Lopez-Villafuerte L, Garcia-Lopez M. Double-blind comparison of azelaic acid and hydroquinone in the treatment of melasma. Acta Derm Venereol Suppl (Stockh) 1989; 143: 58-61.
13. Lawrence N, Cox SE, Brody HJ. Treatment of melasma with Jessner’s solution versus glycolic acid: a comparison of clinical efficacy and evaluation of the predictive ability of Wood’s light examination. J Am Acad Dermatol 1997; 36: 589–93.
14. Khunger N. Newer peels. In: Khunger N, editor. Step by Step Chemical Peels. 2nd edn. Delhi, India: Jaypee Brothers; 2014. p. 149.
15. Sharquie KE, Al-Tikreety MM, Al-Mashhadani SA. Lactic acid as a new therapeutic peeling agent in melasma. Dermatol Surg 2005; 31(2): 149–54.
16. Sharquie KE, Al-Tikreety MM, Al-Mashhadani SA. Lactic acid chemical peels as a new therapeutic modality in melasma in comparison to Jessner’s solution chemical peels. Dermatol Surg. 2006; 32: 1429–36.
I have been exploring for a little for any high quality articles or blog posts on this kind of area . Exploring in Yahoo I eventually stumbled upon this website. Reading this information So i?¦m satisfied to show that I’ve a very good uncanny feeling I found out just what I needed. I so much definitely will make certain to do not put out of your mind this web site and provides it a glance on a continuing basis.
gate io
So, if this clinic is now at Radford instead of UH, does that mean that UH gets no money from it now, or what azithromycin pregnancy
To what blood sugar is an a1c of 7 avoid the light scattering and photobleaching issues, the fluorescence life time was determined for what does viagra do to women There were no breast cancer recurrences in this population
brand anastrozole 1mg arimidex 1mg oral arimidex 1mg generic
clomid usa shippments online This is because the foods contain proteins, which are structurally similar to those in pollen, which means IgE developed from, for example, tree pollen proteins cross reacts to closely related homologues in fruit
completely free online dating chat fdating 100 free dating site free best
free dating site free dating sites for single men and women
service essays essay writing service law school essay paper help best essay helper
help writing a narrative essay help with writing essays help writing college essay help writing essay
%random_anchor_text% %random_anchor_text%
%random_anchor_text% .
best custom essay writing cheap essay writing service online essay writing services recommendations what is a good essay writing service
premium essay writing service essay writing service toronto homework essay help hire someone to write my essay
buy an essay online cheap buy cheap essay help with essay papers what is the best custom essay site
what is the best online essay writing service write my history essay what is a good essay writing service personal statement essay help
best online essay writers essay on service urgent essay help essays custom
law essay help cheap custom essay papers are essay writing services legal online essay helper
best essay writers review buy custom essays online online essay writer essay about military service
write my essay 4 me professional essay writing services top 10 essay writing services college essay helper
i need help writing a essay buy college essay custom essay writing help professional essay writing service
the best essay writing services online essay help the help
essay on racism compare and contrast essay help
writing an essay help custom essay paper tok essay
help cheap essay help
essay writing homework help college essay service cheap essay services buy essay papers
help with writing essay best mba essay writing service how to write my
essay top essay writing service
reliable essay writing service professional college application essay writers essay homework help buy college essays online
100% dating site dating free site online eris free downloads chatting apps adult dating
admission essay editing service help me write a essay essay writer cheap i need someone to write my essay
who can write my essay who will write my essay
english essay helper cheap essay services
essay writer reviews write my essay essay writing website reviews higher english critical essay help
easy essay help essay writing services singapore essay help forum college essay online help
need someone to write my essay custom essays cheap write my essay for money write my essay canada
online essay help essay services reviews custom essays for sale custome essay
i need someone to write my essay best essay website what
are good essay writing services essay writing service best
essay help live chat essay help live chat custom essay
cheap write my admission essay
buy essay online for cheap help to write an essay
essay writing help online help writing scholarship essays
You said that terrifically!
best online casino for blackjack casino online bonus online casino no minimum deposit
Great content. Thank you!
buy already written essays online pay someone to do research paper
Fantastic postings. Thank you.
american writers essay write my admission essay write my english essay
Cheers, I value it.
do essays for me hire a writer for an essay pay someone to write my essay for me
best vpn for public wifi windows vpn best vpn for gaming reddit best vpn for home network
vpn windows 10 best vpn for downloading avira phantom vpn what is vpn on windows
chrome vpn extension free best vpn service 2019 best
vpn for mac free avast vpn free license key
chrome vpn extension free best vpn service 2019 best vpn for mac free https://shiva-vpn.com/
how to get vpn free touch vpn best cheap vpn reddit best free vpn for ios
how to get vpn free touch vpn best cheap vpn reddit https://superfreevpn.net/
best vpn router buy a vpn server free mexican vpn unlimited free vpn – hola
best vpn router buy a vpn server free mexican vpn https://free-vpn-proxy.com/
best free vpn for windows 10 free vpn for firestick
free vpn for netflix free lifetime vpn
best free vpn for windows 10 free vpn for firestick free vpn for
netflix https://rsvpnorthvalley.com/
best multi device vpn best vpn for business vpn vanish best vpn for pc free download
best multi device vpn best vpn for business vpn vanish https://freehostingvpn.com/
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
Azithromycin 250 mg tablets, want considered a “drug of last place to turn,” kills before preventing bacteria from building apartment walls. It binds to wall-building protein fragments called peptides, in particular those that goal with two copies of the amino acid D-alanine (D-ala).
Azithromycin will be in your system for around 15.5 days, after the last dose. Azithromycin walmart has an elimination half-life of 68 hours.
Cenforce tablet. Consulting your doctor reinforces the idea that sexual health is a multidimensional aspect of overall well-being that deserves attention, care, and professional guidance.
Azithromycin 1000mg. Modern equipment facilitates the production of pediatric and geriatric formulations with specialized dosing options.
Automated coding and marking machines print essential information, such as expiration dates and batch numbers, on medication packaging. Azithromycin brand names
Your article gave me a lot of inspiration, I hope you can explain your point of view in more detail, because I have some doubts, thank you.
side effects of plaquenil 200 mg tablets. Medication safety reviews should include assessments of patient preferences for medication brands and generic equivalents.
Institutions should underscore the importance of patient education and empowerment in medication management, encouraging active participation in one’s healthcare journey. is Azithromycin a steroid
ivermectin stromectol where to buy. Stromectol’s mode of action, which targets the nervous systems of parasites, ensures a highly specific and targeted approach to treatment.
ivermectin for cats. Furthermore, the use of Stromectol for lice underscores the value of diversity in healthcare research and treatment options. Health conditions like lice infestations affect individuals from various backgrounds, and the availability of diverse treatment choices ensures that healthcare is inclusive and responsive to the needs of diverse populations. This approach aligns with the principles of health equity, recognizing that healthcare should be accessible and effective for everyone, regardless of their individual circumstances.
how to take dapoxetine 60 mg. Physical causes of ED include conditions that affect blood flow to the penis, such as cardiovascular disease, diabetes, and obesity. Treating these underlying conditions through lifestyle changes, medication, or surgery can often improve erectile function.
Наш интернет магазин создан для того чтобы удовлетворить потребности в стабилизаторах напряжения самых тербовательных клиентов. Заказав у нас стабилизатор напряжения Вы получите не только качественный товар, но и бесплатную доставку по г. Ростов-на-Дону, г. Батайску, г. Аксаю, а также в ближайшие населенные пунткты. И самое главное — все это Вы получите по самым привлекательным ценам. Следите за Горячими предложениями нашего интернет-магазина!!!
стабилизаторы напряжения http://stabrov.ru.
viagra reviews Without enough hormones to produce a five day bleed, you haven t replaced enough estrogen and progesterone to protect your brain and breasts
Healthcare providers should educate patients about potential risks associated with medication storage in homes with young children. ventolin inhaler for sale
Vacuum conveying systems enable the gentle transfer of powders and granules, minimizing material degradation. budesonide 200 mcg
Zithromax is not recommended for use in people with liver or kidney disease, as it can cause these conditions to worsen. azithromycin (zithromax) over the counter.
How long does it take for Ventolin to start working ventolin hfa inhaler.
How do I make him jealous and commit cialis price.
side effects of metronidazole 500 mg Can I take my prescription medication with specific types of protein shakes?
stromectol 3mg tablets. Equipment for lyophilized cake analysis ensures the quality of freeze-dried products.
The Role of AI in Disease Diagnosis and Treatment. Tadalafil liquid
The environmental impact of manufacturing hydroxychloroquine sulfate is an emerging concern. Hydroxychloroquine production challenges us to consider ecological footprints in pharmaceutical manufacturing, aiming for sustainability in health solutions.
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
The accessibility of buy stromectol ivermectin, featuring ivermectin, has been crucial in the fight against river blindness (onchocerciasis) in endemic regions. Mass drug administration programs, supported by organizations like the World Health Organization (WHO), aim to eliminate the disease by distributing ivermectin to at-risk populations, preventing transmission and alleviating suffering.
In the realm of aquaculture, stromectol 3mg, containing ivermectin, offers an effective means of controlling parasitic infestations in fish farms. By mitigating the impact of ectoparasites such as sea lice and gill maggots, it promotes healthier fish populations and sustainable aquaculture practices, thereby supporting food security and economic development.
qiyezp.com
그는 여전히 약간 걱정했습니다. “내시 샤오, 폐하께서는 왕세자를 어떻게 대하십니까?”
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
cenforce 100 mg
fildena
What role does the use of machine learning play in predicting and preventing production errors kamagra online?
How do extended-release pills work how can i compare vidalista 10 to tadarise 10mg?
SightCare formula aims to maintain 20/20 vision without the need for any surgical process. This supplement is a perfect solution for people facing issues as they grow older. https://sightcare-web.com/
WeJiJ is here to help get you the best gaming setup, gaming PC and guide you through the games you like to play with news, reviews and guides. https://wejij.com/
Find the latest technology news and expert tech product reviews. Learn about the latest gadgets and consumer tech products for entertainment, gaming, lifestyle and more. https://axget.com/
Easier WWW is a leading technology site that is dedicated to produce great how-to, tips and tricks and cool software review. https://easierwww.com/
KeraBiotics is a meticulously-crafted natural formula designed to help people dealing with nail fungus. This solution, inspired by a sacred Amazonian barefoot tribe ritual https://kerabiotics-web.com/
Nagano Lean Body Tonic is a groundbreaking powdered supplement crafted to support your weight loss journey effortlessly. https://naganotonic-try.com/
Sugar Defender is a natural supplement that helps control blood sugar levels, lower the risk of diabetes, improve heart health, and boost energy. https://sugardefender-web.com/
– Shoot MASSIVE Loads For An Amazing Finish! https://semenax-try.com/
ZenCortex Research’s contains only the natural ingredients that are effective in supporting incredible hearing naturally.A unique team of health and industry professionals dedicated to unlocking the secrets of happier living through a healthier body. https://zencortex-try.com/
Serolean, a revolutionary weight loss supplement, zeroes in on serotonin—the key neurotransmitter governing mood, appetite, and fat storage. https://serolean-web.com/
Tonic Greens is a ready-made greens shake designed to support the entire body and wellness of the mind. It is filled with over 50 individual vitamins https://tonicgreens-try.com/
MenoPhix is a menopause relief supplement featuring a blend of plant extracts to target the root cause of menopause symptoms. https://menophix-web.com/
BalMorex Pro is an exceptional solution for individuals who suffer from chronic joint pain and muscle aches. With its 27-in-1 formula comprised entirely of potent and natural ingredients, it provides unparalleled support for the health of your joints, back, and muscles. https://balmorex-try.com/
Support the health of your ears with 100% natural ingredients, finally being able to enjoy your favorite songs and movies https://quietumplus-try.com/
Peak BioBoost is a revolutionary dietary supplement that leverages the power of nature to support and improve your digestive system. https://peakbioboost-web.com/
GutOptim is a digestive health supplement designed to support your gut and stomach. It restore balance in gut flora and reduce the symptoms of digestive disorders. https://gutoptim-try.com/
Burn Boost Powder™ is a proven weight loss powder drink that helps to lose weight and boosts the overall metabolism in the body. https://burnboost-web.com
Are there limitations on the frequency of prescription refills with insurance order Cenforce sale?
FlowForce Max is an innovative, natural and effective way to address your prostate problems, while addressing your energy, libido, and vitality. https://flowforcemax-web.com/
CLINICALLY PROVEN* To Increase Semen Volume And Intensity https://semenax-try.com/
DuoTrim is an innovative weight loss supplement that utilizes the power of natural plants and nutrients to create CSM bacteria https://duotrim-us.com/
BioFit is a Nutritional Supplement That Uses Probiotics To Help You Lose Weight https://biofit-web.com/
Dentitox Pro is a liquid dietary solution created as a serum to support healthy gums and teeth. Dentitox Pro formula is made in the best natural way with unique, powerful botanical ingredients that can support healthy teeth. https://dentitox-us.com/
Sugar Balance is an ultra-potent blood sugar supplement that you can use to help control glucose levels, melt away fat and improve your overall health. https://sugarbalance-us.com/
PureLumin Essence is a meticulously-crafted natural formula designed to help women improve the appearance of age spots. https://pureluminessence-web.com/
Alpha Tonic is a powder-based supplement that uses multiple natural herbs and essential vitamins and minerals to help optimize your body’s natural testosterone levels. https://alphatonic-web.com
VivoTonic™ is a 11-in-1 vital blood sugar support formula that may improve how the metabolism goes after the calories that consumers eat. https://vivotonic-web.com/
Progenifix is designed to help maximize weight loss results using a mixture of natural, science-backed ingredients. The formula also has secondary benefits, including promoting overall wellness and vitality and assisting your immune system. https://progenifix-web.com/
AquaPeace is an all-natural nutritional formula that uses a proprietary and potent blend of ingredients and nutrients to improve overall ear and hearing health and alleviate the symptoms of tinnitus. https://aquapeace-web.com
FoliPrime is a simple serum containing a blend of vitamins designed to boost hair health. FoliPrime has 100 percent natural substances that enhance and supplement the vitamins in the scalp to promote hair growth. https://foliprime-web.com/
Gut Vita™ is a daily supplement that helps consumers to improve the balance in their gut microbiome, which supports the health of their immune system. It supports healthy digestion, even for consumers who have maintained an unhealthy diet for a long time. https://gutvita-us.com/
Neuro-Thrive is a brain health supplement that claims to promote good memory and thinking skills and better quality sleep. This nootropic supplement achieves its cause with its potent blend of natural compounds and extracts that are proven to be effective in sharpening mental acuity. https://neurothrive-web.com/
Fast Lean Pro is a herbal supplement that tricks your brain into imagining that you’re fasting and helps you maintain a healthy weight no matter when or what you eat. It offers a novel approach to reducing fat accumulation and promoting long-term weight management. https://fastleanpro-web.com/
The ProNail Complex is a meticulously-crafted natural formula which combines extremely potent oils and skin-supporting vitamins. https://pronailcomplex-web.com/https://pronailcomplex-web.com/
Erectin is a clinically-proven dietary supplement designed to enhance male https://erectin-web.com/
100% Natural Formula Expressly Designed to Help Control Blood Sugar Levels, Improve Insulin Response And Support Overall Health https://glucotrusttry.com/
PowerBite stands as an innovative dental candy, dedicated to nurturing healthy teeth and gums. Infused with a potent formula, it champions the cause of a robust and radiant smile. Crafted meticulously https://powerbite-web.com/
Protoflow is a prostate health supplement featuring a blend of plant extracts, vitamins, minerals, fruit extracts, and more. https://protoflow-web.com/
Unlock the incredible potential of Puravive! Supercharge your metabolism and incinerate calories like never before with our unique fusion of 8 exotic components. Bid farewell to those stubborn pounds and welcome a reinvigorated metabolism and boundless vitality. Grab your bottle today and seize this golden opportunity! https://puravive-web.com/
Zoracel is an extraordinary oral care product designed to promote healthy teeth and gums, provide long-lasting fresh breath, support immune health, and care for the ear, nose, and throat. https://zoracel-web.com
Cerebrozen is an excellent liquid ear health supplement purported to relieve tinnitus and improve mental sharpness, among other benefits. The Cerebrozen supplement is made from a combination of natural ingredients, and customers say they have seen results in their hearing, focus, and memory after taking one or two droppers of the liquid solution daily for a week. https://cerebrozen-try.com/
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
The human body can continue to live thanks to the correct functioning of certain systems. If even one of these systems does not work properly, it can cause problems in human life. https://calmlean-web.com/
Zeneara is marketed as an expert-formulated health supplement that can improve hearing and alleviate tinnitus, among other hearing issues. https://zeneara-web.com/
GlucoBerry is one of the biggest all-natural dietary and biggest scientific breakthrough formulas ever in the health industry today. This is all because of its amazing high-quality cutting-edge formula that helps treat high blood sugar levels very naturally and effectively. https://glucoberry-web.com/
Pineal XT is a revolutionary supplement that promotes proper pineal gland function and energy levels to support healthy body function. https://pinealxt-web.com/
Introducing TerraCalm, a soothing mask designed specifically for your toenails. Unlike serums and lotions that can be sticky and challenging to include in your daily routine, TerraCalm can be easily washed off after just a minute. https://terracalm-web.com/
Are there specific guidelines for importing homeopathic medications from India buy advair?
VidaCalm is an all-natural blend of herbs and plant extracts that treat tinnitus and help you live a peaceful life. https://vidacalm-web.com/
Are you tired of looking in the mirror and noticing saggy skin? Is saggy skin making you feel like you are trapped in a losing battle against aging? Do you still long for the days when your complexion radiated youth and confidence? https://refirmance-web.com/
Gorilla Flow prostate is an all-natural dietary supplement for men which aims to decrease inflammation in the prostate to decrease common urinary tract issues such as frequent and night-time urination, leakage, or blocked urine stream. https://gorillaflow-web.com
HoneyBurn is a revolutionary liquid weight loss formula that stands as the epitome of excellence in the industry. https://honeyburn-web.com/
Keravita Pro™ is a dietary supplement created by Benjamin Jones that effectively addresses nail fungus and hair loss, promoting the growth of healthier and thicker nails and hair. The formula is designed to target the underlying causes of these health issues and provide comprehensive treatment. https://keravitapro-web.com
Volca Burn is a weight loss supplement that uses a “red tingle hack” to help you rapidly lose weight without dieting or exercising. https://volcaburn-web.com/
Xitox’s foot pads contain a combination of powerful herbs that help provide a soothing experience for your feet after a long day. https://xitox-web.com/
Hydrossential is actually a skincare serum or you can say a skincare supplement created by Emma Smith to help women keep their skin looking beautiful and flawless. https://hydrossential-web.com/
Carbofix is the revolutionary dietary formula that promises to activate weight loss without all the extra hard work. https://carbofix-try.com
Reliver Pro is a dietary supplement formulated with a blend of natural ingredients aimed at supporting liver health
Abdomax is a nutritional supplement using an 8-second Nordic cleanse to eliminate gut issues, support gut health, and optimize pepsinogen levels. https://abdomax-web.com
Arctic blast is a powerful formula packed with natural ingredients and can treat pain effectively if you’re struggling with chronic pain. You can say goodbye to muscle cramps with this natural pain reliever in less than a minute. It helps with arthritic pain, blood circulation, and joint pain. It gives long-lasting effects that replace the need to go to surgery. https://arcticblast-web.com
LipoSlend is a liquid nutritional supplement that promotes healthy and steady weight loss. https://liposlend-web.com/
Metabo Flex® Is a Dietary Supplement Formulated Using a Proprietary Blend Of Six Rainforest Super Nutrients And Plants Designed To Boost Metabolism And Reduce Weight. https://metaboflex-us.com
InchaGrow is a new natural formula that enhances your virility and allows you to have long-lasting male enhancement capabilities. https://inchagrow-web.com
Cardio Shield positions itself as an all-encompassing heart health dietary aid. It endeavors to stabilize blood pressure, balance cholesterol levels, and fortify overall cardiovascular health. . https://cardioshield-web.com/
Keratone addresses the real root cause of your toenail fungus in an extremely safe and natural way and nourishes your nails and skin so you can stay protected against infectious related diseases. https://keratone-web.com/
ProstaBiome is a carefully crafted dietary supplement aimed at promoting prostate health. Bid farewell to restless nights and discomfort with ProstaBiome precise strategy for addressing prostate concerns. https://prostabiome-web.com/
PotentStream is designed to address prostate health by targeting the toxic, hard water minerals that can create a dangerous buildup inside your urinary system It’s the only dropper that contains nine powerful natural ingredients that work in perfect synergy to keep your prostate healthy and mineral-free well into old age. https://potentstream-web.com/
Cacao Bliss is a powder form of unique raw cacao that can be used similarly to chocolate in powder form but comes with added benefits. It is designed to provide a rich and satisfying experience while delivering numerous health benefits. https://cacaobliss-web.com/
Payments Latest provides in-depth journalism and insight into the most impactful news and trends shaping payments. https://paymentslatest.com/
Utilitylatest provides news and analysis for energy and utility executives. We cover topics like smart grid tech, clean energy, regulation, generation, demand response, solar, storage, transmission distribution, and more. https://utilitylatest.com
9 da auto news – https://9-da.com/
scshlj banking finance news – https://scshlj.com
dtmliving multifamily news – https://dtmliving.com/
Cneche provides in-depth journalism and insight into the most impactful news and trends shaping the finance industry. https://cneche.com/
Lasixiv provides news and analysis for IT executives. We cover big data, IT strategy, cloud computing, security, mobile technology, infrastructure, software and more. https://lasixiv.com
Wedstraunt has the latest news in the restaurant industry, covering topics like consumer trends, technology, marketing and branding, operations, mergers https://wedstraunt.com
Qcmpt provides in-depth journalism and insight into the news and trends impacting the customer experience space. https://qcmpt.com/
Cneche provides in-depth journalism and insight into the most impactful news and trends shaping the finance industry. https://cneche.com/
Sinohuiyuan provides in-depth journalism and insight into the news and trends impacting facilities management https://sinohuiyuan.com
NordinV provides in-depth journalism and insight into the news and trends impacting the fashion
Huzad delivers the latest news in the grocery industry, with articles covering grocery delivery, online food shopping, shopper behavior, store formats, technology, and more. https://huzad.com/
Grpduk provides news and analysis for human resource executives. We cover topics like recruiting, HR management, employee learning https://grpduk.com
iwinpak provides in-depth journalism and insight into the news and trends impacting the manufacturing sector https://iwinpak.com/
Mscherrybomb provides in-depth journalism and insight into the most impactful news and trends shaping the trucking industry. https://mscherrybomb.com/
Janmckinley provides news and analysis for waste and recycling executives. We cover topics like landfills, collections, regulation, waste-to-energy, corporate news, fleet management, and more. https://janmckinley.com
Serdar Akar provides in-depth journalism and insight into the news and trends impacting the packaging manufacturing space https://serdarakar.com/
Ladarnas provides in-depth journalism and insight into the news and trends impacting the convenience store space. https://ladarnas.com
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://omiyabigan.com/
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://mimsbrook.com
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://sokograd.com
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://bxbinc.com/
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://hostalmindanao.com
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://mariscosleomar.com/
Sugar Defender is a revolutionary blood sugar support formula designed to support healthy glucose levels and promote natural weight loss. https://blackboxvending.com/
Sugar Defender is a revolutionary blood sugar support formula designed to support healthy glucose levels and promote natural weight loss. https://mineryuta.com
Sugar Defender is the rated blood sugar formula with an advanced blend of 24 proven ingredients that support healthy glucose levels and natural weight loss. https://ibcbellows.com/
Sugar Defender is a revolutionary blood sugar support formula designed to support healthy glucose levels and promote natural weight loss. https://acmesignz.com/
sugar defender: https://novabeaute.com/
sugar defender: https://abmdds.com/
sugar defender: https://peyfon.com/
sugar defender: https://nilayoram.com/
sugar defender: https://seahorsesoap.com/
sugar defender: https://sourceprousa.com/
sugar defender: https://royalforestlaundry.com/
sugar defender: https://luckysloader.com/
sugar defender: https://lindadicesare.com/
sugar defender: https://drdenisemichele.com/
sugar defender: https://alchemyfashiongroup.com/
sugar defender: https://bridgerealtysc.com/
geinoutime.com
그러므로… 감히 집에 있지 말고, 감히 목욕을 하지 말고, 감히 긴장을 풀지 마십시오.
geinoutime.com
그는 Xu Pengju의 불순종을 한눈에 볼 수있는 것처럼 Xu Pengju를 흘끗 보았다.
ケロロ軍曹(V2.2)
この記事の情報は計り知れないほど価値があります。大変感謝しています。
魔法少女まどか☆マギカ (2発1)(V2.2)
この記事のおかげで新しい視点を得ることができました。感謝します。
Can a healthcare provider prescribe a branded medicine for psychiatric conditions based on patient preferences safe vidalista dosage?
How do I find a 24-hour pharmacy near me sildenafil buy online?
프라그마틱 슬롯 추천
Xiao Jing은 짜증이났습니다.
777 슬롯
Hongzhi 황제는 Fang Jifan의 말에 매우 동의하는 것 같았고 고개를 끄덕이는 것을 도울 수 없었습니다.
cab 토토
Fang Jifan은 진지하게 고개를 저으며 “폐하, 이것은 콩을 군인으로 바꾸는 것이 아닙니다. “라고 말했습니다.
Can pharmacies legally sell medicines for use in specific medical procedures or surgeries generic loniten?