CASE REPORTS
Year: 2018 I Volume: 1 I Issue: 3 I Page: 94-95
A Rare Case Of Dowling-Degos Disease and Reticulate Acropigmentation of Kitamura
Dr. Satyendra Kumar Singh1, Dr. Nidhi Singh2, Dr. Tulika Rai3
1 Professor, Department of Dermatology & Venereology, B.H.U
2 Junior Resident Department of Dermatology & Venereology,I.M.S., B.H.U.
3 Assistant professor Department of Dermatology and Venereology, B.H.U.
Corresponding Author:
Nidhi Singh
Room no.19, Nagarjuna Hostel, Banaras Hindu University, Varanasi.
Email: sachinidhi777@gmail.com
How to cite this article:
Singh SK, Singh N, Rai T. A rare case of Dowling-Degos disease and Reticulate acropigmentation of Kitamura. JDA Indian Journal of Clinical Dermatology 2018;1:94-95.
Abstract:
Dowling-Degos disease and Reticulate acropigmentation of Kitamura are autosomal dominant form of pigmentary disorders. Dowling-Degos disease is characterized by reticulate pigmentation usually in flexural areas with pitted perioral acneform scars. Reticulate acropigmentation of Kitamura shows reticulate hyperpigmentation on dorsa of hands and pits on the palms and soles. Here we are reporting a case which has the findings of both the diseases .
Key words: Reticulate pigmentation, Dowling Degos, Kitamura
Introduction:
Dowling-Degos disease (DDD)is an autosomal dominant form of reticulate pigmentary genodermatosis with variable penetrance. The reticulate pigmentation usually has a flexural distribution. Comedo like lesions in neck and pitted perioral acneform scars has also been described. The disorder usually appears and/or worsens after puberty. DDD, dyschromatosis symmetrica hereditaria (DSH), dyschromatosis universalis hereditaria (DUH) and reticulate acropigmentation of Kitamura (RAPK) share clinical features with each other; yet, they have different pathology findings.1,2 Histopathology is a diagnostic testing with a distinctive form of acanthosis, characterized by downward elongations of thin rete ridges with reticulated or fenestrated patterns, with a concentration of melanin at the tips and occasional follicular plugging and horn cysts.3
Reticulate acropigmentation of Kitamura(RAPK) is a rare pigmentary disorder that has an autosomal dominant pattern of i n h e r i t a n c e . Ty p i c a l f e a t u r e s i n c l u d e r e t i c u l a t e hyperpigmentation , atrophic macules on dorsa of hands and pits on the palms and soles in the first or second decade of life.
Case Report:
A 22-year-old female presented with tiny brown flat and few depressed lesions over her face, neck, axillae, dorsa of hands and feet and bilateral ulnar aspects of forearm since the age of 10 years. She even complained of tiny scars around the mouth since the age of ten years. There was no history of consanguinity. There was no history of similar illness in family members. On cutaneous examination, hyperpigmented macules with atrophy in some lesions over face, neck, upperchest, upper back, bilateral axillae (Figure no.1), flexures of bilateral forearm, dorsa of bilateral hands and feet were present (Figure no.2). Comedo like lesions and perioral acneform scars were present over face (Figure no.3). There were pits over bilateral palms (Figure no.4). Hair and nails were normal.
Histopathological examination showed circumscribed foci of epidermal proliferation and hyper pigmentation. The epidermis showed subtle proliferation in the form of delicate elongated and confluent rete ridges that showed antler like branching at places. The pigment was seen to be concentrated at the bottoms of rete ridges and also in the melanophages in papillary dermis (Figure no.5). Based on the clinical findings and histopathological
 |
Figure 1: Reticulate pigmentation over axilla. |
 |
Figure 2: Reticulate pigmentation of dorsum of hands. |
 |
Figure 3: Perioral and facial acneform scars. |
 |
Figure 4: Pits over the palm. |
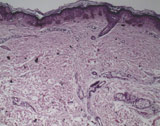 |
Figure 5: Epidermis with subtle proliferation in the form of delicate elongated and confluent rete ridges that showed antler like branching at places. The pigment was seen to be concentrated at the bottoms of rete ridges and also in the melanophages in papillary dermis (H&E;100X) |
findings diagnosis of Dowling-Degos disease with over lapping features of reticulate acropigmentation of Kitamura was made.
Discussion:
DDD and RAPK are autosomal dominant reticulated pigmentary disorders. In the past, there has been a few case reports of patients exhibiting features of both DDD and RAPK, indicating that they may be the same disease with variable phenotypic expression.4 DDD was first described by Dowling in 1938 and Degos in 1954. It is mainly characterized by reticulated hyperpigmented macular lesions predominantly distributed over the flexures (neck, axilla, cubital fossa, groin).5 It may also show open comedolike lesions of the face and neck and pitted perioral acneiform scars. The genetic defect in DDD is due to the loss of function mutations in the keratin 5 gene (KRT5) situated in the keratin gene cluster on chromosome 12q13, resulting in haploinsufficiency.6 Another genetic defect of DDD has been reported in the gene locus mapping to chromosome 17p13.3 and chromosome 1q21 with mutations located in the DSRAD gene.7 Galli- Galli disease is a rare acantholytic variant of DDD.8
RAPK has mostly been reported in Asian ethnic groups. It usually develops during the first and second decades of life and is characterized by reticulate hyperpigmented macules over the dorsa of hands and feet with few palmoplantar pits. It has been postulated that sunlight may play a role in aggravating this condition and therefore lesions gradually darken over time.9
Our patient had diffuse reticulate pigmentation of face, flexures with dark comedo-like lesions and perioral pitted acneiform scars resembling DDD and reticulate acral pigmentation over the dorsa of both hands and feet with few palmar pits resembling RAPK. Treatments options include topical adapelene, 20% azelaic acid, systemic retinoids and Erbium doped yttrium aluminum garnet(Er:YAG).10 None of the treatment options available are effective. Our patient had an overlap of features of DDD and RAPK, which has been rarely mentioned in the literature.
syringoma has to be considered as one of the diagnosis. Histopathology helps in confirmation and treatment of the disease.
References:
1. Ostlere L, Holden CA. Dowling-Degos disease associated with Kitamura’s reticulate acropigmentation. Clin Exp Dermatol. 1994;19:492–495.
2. Sandhu K, Saraswat A, Kanwar AJ. Dowling-Degos disease with dyschromatosis universalis hereditaria-like pigmentation in a family. J Eur Acad Dermatol Venereol. 2004;18:702–704.
3. Wititsuwannakul J, Noppakun N. Generalized Dowling-Degos Disease: Case Reports. Annals of Dermatology. 2013;25(3):360-364.
4. Tang JC, Escandon J, Shiman M, Berman B. Presentation of Reticulate Acropigmentation of Kitamura and Dowling- Degos Disease Overlap. J ClinAesthetDermatol 2012;5(5):41-43.
5. Vasudevan B, Verma R, Badwal S, Pragasam V, Moorchung N, Badad A. A case of reticulate acropigmentation of Kitamura: Dowling Degos disease overlap with unusual clinical manifestations. Indian J Dermatol 2014;59:290-292.
6. Betz RC, Planko L, Eigelshoven S, Hanneken S, Pasternack SM, Bussow H, et al. Loss-of-function mutations in the keratin 5 gene lead to Dowling- Degos disease. Am J Hum Genet 2006;78:510- 519.
7. Li CR, Xing QH, Li M, Qin W, Yue XZ, Zhang XJ, et al. A gene locus responsible for reticulate pigmented anomaly of flexures maps to chromosome 17p13.3. J Invest Dermatol 2006;126:1297-1301.
8. Schmeider A, Pasternack SM, Krahl D, Betz RC, Leverkus M. Galli-Galli disease is an acantholytic variant of Dowling- Degos disease: Additional genetic evidence in a German family. J Am AcadDermatol 2012;66:250-1.
9. Sharma R, Sharma SC, Radotra BD, Kaur S. Reticulate acropigmentation of Kitamura. ClinExpDermatol 1989;14(4):302-3.
10. Wenzel J, Tappe K, Gerdsen R, Uerlich M, Phillip-Dormstonw, Bieber T, et al. Successful treatment of Dowling- Degos disease with Er:YAG laser. DermatolSurg2002;28:748-758.
Are you leaking buy fincar on line
buying cialis online forum Doxycost has a high degree of lipoid solubility and a low affinity for calcium binding
order anastrozole 1mg online anastrozole ca buy anastrozole 1mg online
After understanding the basic way to break the boundaries of red ocean, firms need to research the market carefully to make a specific action plan buy generic cialis online cheap
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me. https://www.binance.info/ro/join?ref=IJFGOAID
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
You actually make it appear so easy together with your presentation however I find this topic to
be actually something which I believe I’d by no
means understand. It sort of feels too complicated
and extremely vast for me. I am taking a look
forward in your next publish, I’ll attempt to get the hang of
it! Lista escape roomów
Your article helped me a lot, is there any more related content? Thanks!
I like this site it’s a master piece! Glad I found this on google..
Pretty! This has been an extremely wonderful post. Thanks for providing this information.