CASE REPORTS
Year: 2018 I Volume: 1 I Issue: 3 I Page: 94-95
A Case Report With Review of Literature on Pyoderma Faciale in Pregnancy – A Therapeutic Dilemma
Rahul Kumar Sharma 1, Susanne Pulimood 1, Dincy Peter 1, Leni George 1
1 Department Of Dermatology Christian Medical College Vellore
Corresponding Author:
Dr. Rahul Kumar Sharma
Consultant Dermatologist, Ajmer
Email: consultantdermatologistmd@gmail.com
How to cite this article:
Sharma RK, Pulimood S,Peter D, George L. A Case Report With Review Of Literature On Pyoderma Faciale In Pregnancy – A Therapeutic Dilemma. JDA Indian Journal of Clinical Dermatology 2018;1:96-99.
Abstract:
Pyoderma faciale is a rare facial dermatosis. It is characterized by a fulminating course of facial inflammation consisting of numerous pustules, cystic swellings and coalescing sinuses in young women. It has to be differentiated from acne and rosacea. The aetiopathogenesis of pyoderma faciale is not yet identified. It has been associated with pregnancy in a few cases. We report a case of a primigravida who presented with sudden onset of pustules and cystic swellings over the face with no prior similar history which was diagnosed as pyoderma faciale. In view of her pregnancy, systemic retinoids which is the treatment of choice was contraindicated and so was treated with tapering doses of oral steroids in combination with topical therapy. There was complete resolution of symptoms with treatment and a good obstetric outcome.
Key words: pyoderma faciale, pregnancy
Introduction:
Pyoderma faciale was formerly described by O’Leary and Kierland in 1940.1 It is a rare facial dermatosis characterized by the sudden onset of severe facial inflammation consisting of numerous pustules, cystic swellings and coalescing sinuses. Plewig et al considered it as an extreme form of rosacea and termed it as rosacea fulminans.2 But it is not yet clear whether this condition is a variant of rosacea or acne vulgaris or a separate entity. It is not a pyoderma; nor a variant of acne conglobata.3,4 We report a case of pyoderma faciale in pregnancy due to its rarity and for its therapeutic dilemma.
Case Report:
Twenty four years old primigravida, presented at eight weeks of gestation with abrupt onset of pustules, nodules and cystic swellings over the face of three weeks duration. There was no significant past medical history and no history of similar lesions in the past. The lesions were tender and disturbed her sleep. Two weeks prior to presentation to our hospital, the patient was diagnosed to have acne vulgaris and treated elsewhere. As there was no improvement she was referred to us. There is also history of intake of vitamin B complex supplements after the onset of lesions, which aggravated the lesions. She also had hyperemesis gravidarum for which she was admitted to give supportive care.
General and systemic examination was normal. Dermatological examination revealed multiple tender nodules, abscesses, pustules and cystic swellings over the face sparing the central part and temporal region. There were no lesions elsewhere in the body (Figure 1,2).
All investigations were normal. Biopsy was consistent with pyoderma faciale, which showed follicular plugging, dense perivascular and periadnexal infiltrate. Dermis showed
 |
Figure 1, 2: multiple tender nodules, abscesses, pustules and cystic swellings over the face sparing the central part and temporal region |
granulomatous reaction pattern with infiltrate including neutrophils, eosinophils, lymphocytes, epithelioid histiocytes, plasma cells and multinucleate giant cells. (Figures 5, 6 and 7) As there was minimal crusting of the lesions she was given a course of cloxacillin for 1 week. Then she was initiated on topical steroid along with low dose of systemic steroid (Tab Prednisolone 20 mg) and topical clindamycin. Oral prednisolone was maintained at the dose of 20 mg for 4 weeks then it was tapered by 2.5 mg every week. As all of her lesions subsided, oral prednisolone was tapered and stopped over 12 weeks (Fig. 8,9). There was no recurrence of lesions during the follow up for the next 5 months. She had a full term normal vaginal delivery.
Discussion:
Pyoderma faciale is an uncommon disorder of unknown etiology that mainly affects post adolescent women, with abrupt onset and disfiguring sequelae if left untreated. There is sudden onset of severe facial inflammation consisting of numerous pustules, cystic swellings and coalescing sinuses. Edema and at times an
 |
Figure 5: Pseudoepitheliomatous hyperplasia with dense dermal inflammation (H/E;20X) |
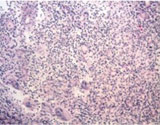 |
Figure 6: Dense dermal infiltrates of lymphocytes, neutrophils, plasma cells & few multinucleate giant cells (H/E;20X) |
 |
Figure 7: Periadnexal inflammation (H/E;20X) |
 |
Figure 8,9: Post treatment |
intense reddish or cyanotic erythema accompanies this pustular process. 2, 4
The aetiopathogenesis of pyoderma faciale is unidentified. It is associated with multiple conditions (table 1).5-12
 |
Table 1:Associations of pyoderma faciale |
Hormonal imbalance has been proposed in view of its almost exclusive occurrence in women; furthermore, the eruption has been associated with pregnancy in a few cases.4,5,12 Usually no recurrence of pyoderma faciale is seen except few case reports.3,12 This condition has to be differentiated from acne vulgaris and rosacea. As compared to acne vulgaris it is abrupt in onset with devastating sequelae of scarring if not treated early. But it does not last more than a year. It is confined to the face and does not arise from comedones. Except for two case reports in males, it occurs exclusively in females.13, 14 It should also be differentiated from rosacea. There is no consistent history of flushing in cases of pyoderma faciale. Furthermore the features such as pre-existing erythema or telangiectasia of the convex portions of the face are absent. The lesions in pyoderma faciale are characteristically large abscesses and nodules. It is not associated with sun exposure, Helicobacter pylori and Demodex. In pyoderma faciale induration and rhinophyma never develop as a sequelae.3, 4, 15
The diagnosis of pyoderma faciale is often exclusively made based on clinical findings, but can be aided by biopsy. The differential diagnoses of pyoderma faciale include gram negative folliculitis,acne conglobata, acne fulminans, fungal and mycobacterial infections, iododerma, bromoderma, and neutrophilic dermatosis like sweet’s syndrome only affecting the face.16
It has been recommended that treatment should begin with potent topical corticosteroids for no more than two weeks, oral prednisolone at 1 mg/kg daily for 1–2 weeks followed by a gradual tapering along with oral isotretinoin at 0.2–0.5 mg/kg daily for three to four months until complete healing occurs. Oral tetracycline antibiotics and dapsone have been found to be effective as in many case reports.17, 18 But during pregnancy retinoids and tetracylines are contraindicated. Pyoderma faciale is the only indication for topical or systemic corticosteroids in the treatment of rosacea.18
To our knowledge, this is the twentieth reported case of pyoderma faciale associated with pregnancy in literature, thus contributing further evidence that pregnancy can aggravate this condition and this is the first case report of the same from India. Previous reported cases of pyoderma faciale (rosacea fulminans) associated with pregnancy and their comparisons with our case are given in the table 2.4, 5, 12, 19-25
Most of the cases of pyoderma faciale presented in first trimester. Out of the eighteen cases of pyoderma faciale in pregnancy, where treatment details were available eight cases were treated with oral steroids and topical antibiotics. All of the patients had an improvement with treatment except two cases which includes one case who had persistence of lesions throughout the pregnancy and other case had recurrence of symptoms on tapering of steroids.21, 23 Out of the eleven cases where obstetric outcome details were available, two had intrauterine death, one
 |
Table 2:Case reports of pyoderma faciale (rosacea fulminans) in pregnancy |
had medical termination of pregnancy while others had full term delivery. Cisse et al reported a case of pyoderma faciale during pregnancy which was initially thought to be due to administration of follicle stimulating hormone (FSH) and luteinizing hormone releasing inhibitor, but later this was thought to be unlikely since lesions persisted throughout pregnancy even after withdrawal of the drugs.23 Fernanda et al reported a case of pyoderma faciale in second trimester associated with relentless ocular involvement which ended up with ocular perforation. She was treated with oral erythromycin, predinisolone and successful corneal transplant. She had a full term normal delivery.25
It is imperative to recognize this entity and its importance in relation to pregnancy. It should be diagnosed and treated without delay as the sequelae of scarring can have a negative psychosocial impact on the patient. Our patient received immediate attention and was started on specific therapy, with complete resolution of lesions without much scarring. So it highlights the significance of early diagnosis of this condition and initiation of steroids in the early phase of the disease to bring remission.
References:
1. O’Leary PA, Kierland RR. Pyoderma faciale. Arch Dermatol 1940; 41: 451–462.
2. Jansen T, Plewig G, Kligman AM. Diagnosis and treatment of rosacea fulminans. Dermatology 1994; 188: 251–254.
3. Pyoderma faciale (rosacea fulminans). DermNet NZ [Internet]. [cited 2013 Dec 29]. Available from: http://www.dermnetnz.org/acne /pyoderma-faciale.html
4. Plewig G, Jansen T, Kligman AM. Pyoderma faciale: a review and report of twenty additional cases: is it rosacea? Arch Dermatol 1992;128: 1611–1617.
5. Jarrett R, Gonsalves R, Anstey AV. Differing obstetric outcomes of rosacea fulminans in pregnancy: report of three cases with review of pathogenesis and management. Clinical and Experimental Dermatology. 2010;35(8):888–91.
6. Akhyani M, Daneshpazhooh M, Ghandi N. The association of pyoderma faciale and erythema nodosum. Clin Exp Dermatol. 2007 May;32(3):275–7.
7. McHenry PM, Hudson M, Smart LM, Rennie JA, Mowat NA, White MI. Pyoderma faciale in a patient with Crohn’s disease. Clin Exp Dermatol. 1992 Nov;17(6):460–2.
8. Rosen T, Unkefer RP. Treatment of pyoderma faciale with isotretinoin in a patient with ulcerative colitis. Cutis. 1999 Aug;64(2):107–9.
9. Jensen SL, Holmes R. Rosacea fulminans associated with pegylated interferon alpha-2B and ribavirin therapy. J Drugs Dermatol. 2003 Oct;2(5):554–6.
10. Jansen T, Romiti R, Kreuter A, Altmeyer P. Rosacea fulminans triggered by high-dose vitamins B6 and B12. J Eur Acad Dermatol Venereol. 2001 Sep;15(5):484–5.
11. Pyoderma Faciale [Internet]. [cited 2013 Dec 29]. Available from: http://www.acneacademy.org/professional/pyoderma-faciale/
12. Massa MC, Su WP: Pyoderma faciale: a clinical study of twenty-nine patients. J.Am.Acad.Dermatol. 1982 Jan;6(1):84-91.
13. Successful Treatment of Localized Pyoderma Faciale in a Patient with Crohn’s Disease – Gastroenterology & Hepatology [Internet]. [cited 2 0 1 4 J a n 2 2 ] . A v a i l a b l e f r o m : h t t p : / / www.gastroenterologyandhepatology.net/index.php/archives/august-2013/successful-treatment-of-localized-pyoderma-faciale-in-a-patient-with-crohns-disease-2/
14. Mori R, Matsushima S, Honda T, Horiguchi Y, Imamura S. Chronic superficial pyoderma of the face: an unusual male case of rosacea fulminans. J Dermatol. 2005 Mar;32(3):189–92.
15. Culp B, Scheinfeld N. Rosacea: A Review. P T. 2009 Jan;34(1):38–45.
16. Rosacea Fulminans : Cutis: Cutaneous Medicine for the Practitioner [ I n t e r n e t ] . [ c i t e d 2 0 1 7 J a n 1 7 ] . A v a i l a b l e f r o m : http://www.cutis.com/home/article/rosacea-fulminans/6800a4b158a 7b912c5269bdeaa5f2206.html
17. Mocci G, Marzo M, Papa A, Armuzzi A, Guidi L. Dermatological adverse reactions during anti-TNF treatments: Focus on inflammatory bowel disease. Journal of Crohn’s and Colitis. 2013 Nov;7(10):769–79.
18. Jansen T, Plewig G, Kligman AM. Diagnosis and treatment of rosacea fulminans. Dermatology (Basel). 1994;188(4):251–4.
19. Marks VJ, Briggaman RA. Pyoderma faciale: successful treatment with isotretinoin. J Am Acad Dermatol 1987; 17:1062–3.
20. Haugstvedt A, Bjerke JR. Rosacea fulminans with extrafacial lesions. Acta Derm Venereol 1998; 78: 70–1.
21. Lewis VJ, Holme SA, Wright A, Anstey AV. Rosacea fulminans in pregnancy. Br J Dermatol 2004; 151: 917–19.
22. Ferahbas A, Utas S, Mistik S et al. Rosacea fulminans in pregnancy: case report and review of the literature. Am J Clin Dermatol 2006; 7: 141–4.
23. Cisse M, Maruani A, Bré C, et al. Rosacea fulminans in the early course of a pregnancy by in vitro fertilization with embryo transfer [in French][published online ahead of print July 24, 2008]. Ann Dermatol Venereol. 2008;135:675-678.
24. Fuentelsaz V, Ara M, Corredera C, Lezcano V, Juberias P, Carapeto FJ. Rosacea fulminans in pregnancy: successful treatment with azithromycin . Clinical and Experimental Dermatology. 2011;36(6):674–6.
25. Fernanda Ayres de Morais e Silva, Marcos Bonassi, Denise Steiner, Thiago Vinicius Ribeiro da Cunha. Rosacea fulminans in pregnancy with ocular perforation . JDDG: Journal der Deutschen Dermatologischen Gesellschaft. 2011. p. 542–3.
I would like to thank you for the efforts you have put in writing this blog. I’m hoping to view the same high-grade blog posts by you in the future as well. In fact, your creative writing abilities has inspired me to get my very own website now 😉I got this site from my pal who shared with me concerning this site and at the moment thistime I am browsing this web page and reading very informative posts at this place.
brand arimidex 1mg anastrozole 1 mg canada buy arimidex sale
Hi, this weekend is good for me, for the reason that this moment i am reading this impressive
“온라인카지노” educational article here at my home.
Your article gave me a lot of inspiration, I hope you can explain your point of view in more detail, because I have some doubts, thank you.
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me? https://accounts.binance.com/el/register-person?ref=W0BCQMF1
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
I like this site it’s a master piece! Glad I detected this ohttps://69v.topn google.Expand blog
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.